A CASE STUDY (Read the
latest events in the case)
HEADLINE:
January 27, 2000 Washington
State Medical Quality Assurance Commission grants Dr. Smith a full medical
license under whistle-blower protection provisions of state law. The
Commission does not require Brigadier General Mack Hill’s signature. Hill continues to refuse to answer the
letters from Quality Assurance Commission about Dr. Smith, a physician who works for him.
![]()
Why is this Army Doctor
under reprisal for reporting JCAHO standards violations?
- What danger to patient
care Dr. Stephen Whitlock Smith reported
- What constituted the
reported reprisal
Who
are the Army Medical Generals accused by Stephen Whitlock Smith, MD, of violating
JCAHO standards?
- Brigadier General Kevin Kiley (Assistant Army Surgeon General) telephone (703)
681-3000
- Brigadier General Mack Hill (first non physician Commander of Madigan Army Medical Center) telephone (253) 968-1190
Could
Brigadier General Kevin Kiley influence Dr Smith's credentials and influence
any investigations?
- Brigadier General Kevin
Kiley is in charge of medical credentials for the Army! Telephone (703) 681-3000.
- Brigadier General Kevin
Kiley has personnel matters including retirements within his sphere of influence.
- Brigadier General Kevin
Kiley is now in charge of the same office which recommended the investigation of his Command!
Who is the one Army Medical General
who can resolve the situation?
- Lieutenant General Ron Blanck, Surgeon General of the Army telephone (703) 681-3000
What Dr. Stephen Whitlock Smith reported:
- Landstuhl Army Regional
Medical Center (LARMC) 1994-1996,
under Command of then Colonel (Promotable) Kevin Kiley
- Orders to emergency
care personnel to abandon care of civilians with unstable medical
conditions, violating Army Regulation 40-3:4-59, LARMC PAM 40-24, JCAHO
standards, and Good Samaritan Practice.
- Suppression of quality
assurance documents reporting violation of standards of Joint Commission
for Accreditation of Healthcare Organizations (JCAHO), not reported to
JCAHO surveyors in May 1996
- Orders for medical
personnel to work in violation of their work limitations, violation of Army
Regulation 40-5
- Diversion of ambulances
to the black market instead of into necessary patient care
- No maintenance for 7
straight years of the emergency beeper system: the contractor received
payment for 3 of those years
- Unnecessary brain
injury in a teenager (Read extract of Hilton Head article) (Read Dr. Smith’s eyewitness account)
- Wrongful death of Baby
Victoria, not reported to JCAHO surveyors
in November 1996
The Reported Reprisal Involved the following:
- Unlawful
psychiatric hospitalization 1996 by order of then COL (Promotable) Kevin
Kiley including violation of DOD Whistleblower Directives, Army Regulation
40-68, and JCAHO standards of due
process. Dr Russell Hicks, telephone (253) 968-3172, current Chief of
Psychiatry at Madigan, has specific knowledge of these events.
- Failure
to investigation in 1996 by LTC Michael Stearns, then COL Kiley’s former Inspector General at
Landstuhl, now Brigadier General Mack Hill’s Inspector General at Madigan,
telephone (253) 968-1190!
- Unlawful
use of a misrepresented psychometric test result (now reported as “never
existing” by BG Hill’s Command) to place Dr Smith under credentials
supervision in April 1997
- Reprisal
against one of Dr. Smith’s witnesses Ms.
Kelly Theriot (Ms Theriot is one of MAMC’s former
medical claims attorneys knowledgeable about a medical claim from LARMC
and the practice status while at MAMC of one of the respondents
- Anger directed toward
Dr Smith by Brigadier General Mack Hill (Kiley’s close associate) in
reprisal for Dr. Smith’s brief conversation with Dr. Sue Bailey, Assistant
Secretary of Defense for Health Affairs, on 1 September 1998
- Reprisal detention and physical
assault by Madigan hospital security agent after Brigadier General Mack Hill’s display of anger toward Dr. Smith
- Dr Russell Hicks,
current Chief of Psychiatry at Madigan at telephone (253) 968-3172,
received a full report of these events from Dr. Smith twice in September,
in his capacity as Dr. Smith’s assigned Army psychiatrist under the
Madigan Impaired Provider Committee. However, the action from that
Committee came not from Dr. Hicks, but from Orthopedist Fred Johnstone,
Chief of Orthopedics who diagnosed Dr. Smith as experiencing “paranoid
delusions.”
- Refusal
by Quality Services Director Nancy Greenfield, RN, telephone (253)
968-2487, on 3 March 1999 and other occasions to remove erroneous and
inappropriate documents from credentials files of Dr. Smith. Ms Greenfield
is currently the principal JCAHO representative at Madigan.
- Continuing denial of
due process in credentialing by BG Mack Hill, close associate of Brigadier
General Kevin Kiley, and Hill’s failure to respond to legal challenge of
credentials JCAHO due process violations.
- Office of the Surgeon
General of the Army, where BG Kiley controls Army credentials, received
the official legal challenge in June 1999; however, no response has been
obtained from that office
- Specific delays in
reestablishing credentials by COL James Gilman,
telephone (253) 968-1190, current Madigan Deputy Commander who reports to
Brigadier General Mack Hill: COL Gilman should explain if he is following Army
Regulation 40-68 and JCAHO due process guidelines in his actions, and
should answer the following questions:
- Why did COL Gilman
delay any actions to allow Dr. Smith to see patients again
until July 16 1999, just days after the Army Times reported the delay,
and more than 4 months after the credentials committee had ordered the
restoration of credentials?
- What does COL Gilman
know about the missing clinic records, not available for the May 10 UW
referral, and what has he done to attempt their retrieval?
- Why
did COL Gilman exclude the Department Chief and the Troop Commander from
the October 4 counseling session, give an adverse evaluation to Dr Smith
not confirmed by the Department Chief, and give denial of emergency loan
request not confirmed by the Troop Commander.
- Why
did COL Gilman not help to avoid Dr. Smith’s current financial and family
emergency?
- Why
is COL Gilman micromanaging Dr. Smith’s supervisory plan, instead of
deferring to the true supervisors?
World
Wide Web Report updated 14 February 2000 after presentation at 11:45 AM on 18
October 1999 at Madigan Army Medical Center to the following:
·
Joint Commission on Accreditation of Healthcare
Organizations Physician Surveyor Dr. Charles Blewett for Dr
Dennis O’Leary, President of JCAHO telephone (630) 792-5000, JCAHO Case #134,
and
·
Department of Defense Inspector General Investigator
Debby Gibson for Donald
Mancuso, Acting Inspector General telephone (800) 424-9098 DODIG Case
#67218/372088, via COL Peterson;
·
COL Peterson, Inspector General, I Corps and Fort Lewis,
telephone (253) 967-5181 was consulted in person on Monday 18 October and
requested to assure safe transfer of protected documents to the JCAHO Physician
Surveyor Dr Charles Blewett, and to Department of Defense Inspector General
Investigator Debby Gibson for Donald Mancuso. COL Peterson accepted the
computer disk of protected documents and agreed to transfer it to DODIG.
Current
Situation
- Stalled
investigations
- Delayed
retirement
- Delayed
restoration of full credentials
- Delayed
verification by MAMC for Washington State licensure
Investigations
- Department of Defense
Inspector General Program Integrity #67218/372088
- General
Accounting Office, Special Investigations #40627
- Office
of Special Counsel #MA-99-1640
- Joint
Commission for Accreditation of Healthcare Organizations #134 (Read
the JCAHO complaint)
- Legal
appeal to LTG Blanck for due process in credentials actions (Read
the Appeal)
Contact
Information
E-mail address
stevewsmith@pol.net, stevewsmith@ephysician.md
Telephone
253-576-6746
Biographical Information
·
Stephen Whitlock Smith,
MD, completed all of his medical training in the Army,
and served in Desert Storm in the Saudi desert near Kuwait
·
Stanford University, Palo Alto, California, 1970
(Biology)
·
George Washington University School of Medicine 1980
(MD, Army Scholarship)
·
Eisenhower Army Medical Center, Internal Medicine
Residency, 1983
·
Madigan Army Medical Center, Emergency Medicine
Residency, 1987
·
Elected Fellow, American College of Physicians, 1994
·
Elected Fellow, American College of Emergency
Physicians, 1991
***************************************************************************
JCAHO and DODIG Summary Letter to Dr Dennis O’Leary and Donald Mancuso
Attention: Dennis
O’Leary, MD, and Donald Mancuso
Gentlemen:
My complaint is contained in this Web site, with confidential documents passed
to you under separate cover on 18 October 1999, anticipatory of assistance from
COL Peterson, Inspector General of I Corps and Fort Lewis. Because of the
complexity of the case and the huge number of documents, I am writing this
outline to point out the key problems and to signal the key documents.
My complaint (JCAHO
#134 and DODIG #67218) can be divided up into several areas:
- JCAHO
standards violations at Landstuhl 1994-1996 under then COL (Promotable)
Kevin Kiley
- Reprisal
against me for my complaint, both at Landstuhl and at Madigan
- Adverse
actions that affect me and my family in a global nature
- Harm
to my professional reputation within Madigan and within the Army and
civilian medical communities
- Risk
to my Army career
- Risk
of adverse action by State Licensing Boards under which I hold current
licenses
- Harm
of publicity to myself and my family
- Financial
devastation from a combination of attorney and physician fees already
paid or billed, in order to defend my credentials and livelihood
($30,000 is the current amount)
- Problems
in obtaining credit for loans to repay the huge debt (I have been unable
to obtain local bank loans to cover the $30,000, since BG Mack Hill has
not restored my full credentials nor signed the verification of my
hospital privileges for Washington State MD Licensing.
- Financial
endangerment of my children’s college prospects because of the debt
- Current
inability to obtain civilian employment as physician in Washington State
without full credentials and without BG Hill’s verification signature
- Emotional
distress to myself and family and friends
- Temporary separation from family
- Need for family interventional psychotherapy, as
recommended by both Dr Dunner and Dr. Hickey
- Due
process violations, especially violations of DOD directives 6490-4 and
6490-1 and their antecedents, Army Regulation 40-68, and JCAHO Medical
Staff guidelines
- By
then COL (Promotable) Kevin Kiley at Landstuhl
- By
officials at Madigan after medical evacuation from Landstuhl
- April
1997 reduction of level of privileging after notification to Commander
by Mike Meines of my whistleblower status
- Documentary
record
- insertions
of misrepresented or falsified material, especially in violation of DOD
IG Directive of Ms Susan J. Crawford of February 1991 and AR 40-68
- important
documents unaccounted for
- Psychometric Test Interpretation by Psychologist LTC
Brad Powell
- Psychology Clinic Records by LTC Powell
- Psychiatry Clinic records by Drs. Marc Williams and
Russell Hicks
- Dr Russell Hick’s reports to the Impaired Provider
Committee of the 1 September 1998 episode of harassment against Dr.
Smith which preceded his episode of depression
- I
am requesting JCAHO and DOD IG assistance in resolving this matter of my
credentials fairly, investigation into my allegations of reckless
endangerment at Landstuhl 1994-96, and full exposure of MAMC’s treatment
of me as a whistleblower.
- I
am today in receipt of the following letter by Mr. Mancuso, sent to me by
Senator Strom Thurmond’s office, which verifies that the DOD IG
investigation into my complaints is ongoing. I quote the letter in its
entirety:
“Inspector General,
Department of Defense, 400 Army Navy Drive, Arlington, VA 22202-2884
Honorable Strom
Thurmond
United States
Senate
Washington, DC
20510-4001
Dear Senator
Thurmond:
This is in response
to your letter of June 22, 1999, regarding Lieutenant Colonel (LTC) Stephen W.
Smith, US Army Medical Corps (case number 372088.) LTC Smith alleged that he is
continuing to suffer reprisals for his 1996 reports of mismanagement at the
Landstuhl Regional Medical Center, Landstuhl, Germany.
“This office has
reviewed a report of investigation from the Inspector General (IG), Department
of the Army, regarding reprisal allegations made by LTC Smith. More recently,
the Army IG has completed its investigation of the allegations of mismanagement
at Landstuhl. Our review of these investigations determined that additional
review and analysis is necessary before we can conclude that all issues raised
by LTC Smith have been adequately addressed. In that regard, we have recently
interviewed LTC Smith and anticipate interviewing other US Army Medical Corps
personnel in the near future. The results of our review of this matter will be
provided to you as soon as possible.
“Please accept our
regrets for the delay in providing you with a more timely interim response. If
we may be of further assistance, please contact me or Mr. John R. Crane, Office
of Congressional Liaison, at (703) 604-8324.
“Sincerely,
Donald Mancuso
Acting Inspector
General”
Finally, Gentlemen,
I remind you that the allegations that I am making herein are extremely serious
because they appear to involve deliberate violations of Army Regulations and
Joint Commission guidelines at Landstuhl 1994-1996 by officers reporting to
then COL Kevin Kiley, and reprisal against me and other witnesses at Madigan at
the apparent direction of Brigadier General Mack Hill, a former close associate
of Brigadier General Kevin Kiley. I do not dispute that I myself became
delinquent in medical records in early September 1998, after the episode of
reprisal detention which followed shortly after an episode of harassing
behavior by BG Hill himself. I reported that I was falling behind in records
and would need additional assistance in order to complete them. However,
Brigadier General Mack Hill and his command utilized both the Impaired Provider
Committee and the Credentials Committee in an apparent reprisal mode against a
whistleblower, and not in the way that Army Regulation 40-68 and JCAHO
guidelines stipulate. Various DOD Directives were also apparently disregarded:
- The
Directive issued in February 1991 by DOD IG Susan J. Crawford to Army
Medical Facilities (Madigan was named specifically) not to place adverse
documentation unrelated to medical credentials into a provider’s
credentials file, and
- DOD
Directives protecting whistleblowers from retaliation (DOD directives
6490-4 and 6490-1 and their antecedents)
Furthermore, both
JCAHO and the DOD IG have an opportunity to investigate irregularities not
previously investigated by the responsible agencies. If uncompleted Army investigations are reactivated by your efforts, that will bring back respect to the
organization that was lost when MG David Hale, an Assistant Army Inspector
General, during the time my complaints were being investigated, was
investigated for Court-Martial.
Some of the criticisms of the Joint Commission that it is too
lenient might be answered to the organization’s
credit if the irregularities which I report do actually force Madigan to follow
established due process Regulations and guidelines, especially in a
whistleblower case.
I can provide
whatever additional material which you require for your investigation.
My item-by-item
appeal to you follows later in this document. (hyperlink
to JCAHO/DOD IG appeal)
Stephen Whitlock
Smith, MD
***************************************************************************
THE
FOLLOWING CONSISTS OF A TIMELINE INCLUDING ALLEGATIONS TO BE INVESTIGATED:
Feb
1991 Following the initial leadership of Senator John Glenn to investigate the
medical administration of the Army in Germany, in Feb 1991, Department of
Defense Inspector General Susan Crawford issues report to then Sen.
William Cohen telephone (703) 697-5737, Sen. Cranston,
and other members of the Senate Armed Services Committee, ordering Army
Physician Commanders to stop utilizing credentials libel to discipline Army
Physicians. The Secretary of the Army is directed to comply. Madigan Army
Medical Center is one of those listed in the report. Two current leaders with
personal knowledge of these events: Secretary
of Defense William Cohen (703) 697-5737, and Brigadier General John Parker,
telephone (703) 681-3000 currently an Assistant Army Surgeon
General reporting to LTG Ron Blanck.
July-August
1993 REPRISAL FOR JOINT COMMISSION COMPLAINT: Landstuhl Deputy Commander COL
David Lipsi and Quality Manager Cliff Wagner allegedly tape record testimony
provided to Joint Commission Physician Inspector Bert Hurowitz, MD. One
Landstuhl physician is ordered to an involuntary psychiatric evaluation one day
after he had made his report to Dr Hurowitz. Two other physicians received
threats from COL Lipsi. Charges against COL Lipsi for alleged credentials libel
and intimidation of witnesses by the physicians' defense attorney are
mysteriously dropped. Into this command environment, COL Kevin Kiley assumed
command of Landstuhl in Summer 1994.
May
1994 LTC David Gillingham, a Madigan Family Practice physician, leaves Madigan
for Landstuhl. What is his credentials standing at this time? (Read the account
of reported reprisals against one of the MAMC
medical claims attorneys knowledgeable of this situation.)
June
1994 As reported by Dr Smith, LTC Gillingham and COL Lipsi order LTC Stephen
Whitlock Smith to falsify a credentials file evaluation, a violation of AR
40-68 and JCAHO standards, in Dr Gillingham's favor; Dr Smith refuses and comes
under reprisal by Landstuhl Command.
June
17 and 19, 1994 As reported by Dr Smith, LTC Gillingham orders a
command-directed mental health evaluation of Dr Smith.
1994-95
As reported by numerous direct witnesses, COL Lipsi and LTC Gillingham quote
direct orders from COL Kiley to ER staff to abandon care of unstable patients.
ER refuses. COL Lipsi and LTC Gillingham inform Dr. Smith that he will forfeit
the dollar amount of a patient’s hospital bill by order of COL Kiley.
May
1995 As memoranda document, Dr Smith and ER Staff warn Colonel (Promotable)
Kevin Kiley about Joint Commission deficiencies likely to cause harm to
patients.
June
3, 1995 Reportedly, LTC Gillingham sends a teenage boy home with written
diagnosis of abrasions; the boy had sustained prolonged loss of consciousness,
had a severe headache, and had no memory of the event (retrograde amnesia.)
June
4, 1995 Teenage boy returns unconscious, herniating, posturing; Dr Smith and ER
staff stabilize him (via intubation, hyperventilation, corticosteroids); LARMC
neurosurgeon is not reported not reachable by beeper or phone. Dr Smith
transfers boy to Kaiserslautern for lifesaving surgery.
June
6 1995 The Newspaper Stars and Stripes makes inquiries about the boy with the
brain injury. COL (Promotable) Kevin Kiley orders through Ms Marie Shaw, his
Public Affairs Chief, that no one talk to the press about the case. The boy’s
father visits LARMC asking questions about the boy’s management. Dr Smith
refers him to LTC Gillingham and COL Lipsi, and calls COL Lipsi to let him know
the boy’s father is on the way to see him. The boy’s father refuses to see LTC
Gillingham, and goes to see COL Lipsi, whose office turns the man away quoting
Quality Assurance confidentiality regulations. The same day, LARMC ER personnel
report that they suspect that the clinical record of the boy’s first day of
treatment at LARMC may have been reconstructed after the fact, with the
original record unaccounted for.
Feb
12, 1996 Dr Smith reports Joint Commission violations to COL Kiley; 2 hours
later, Dr Smith is ordered into "Impaired Provider" program; COL
Russell Hicks is the psychiatrist. Dr. Smith is ordered transferred 7,000 miles
to Madigan for in-patient confinement. Alleged lack of due process in both
credentialing and in reevaluating psychiatric detention are deviations from DOD
directive on improper mental health evaluations, Army Regulation 40-68, and
JCAHO standards of due process for Medical Staff.
Spring,
1996 Landstuhl passes Joint Commission inspection. Subordinates of COL (P)
Kiley allegedly suppressed the cases reported by Emergency Services, including
Quality Assurance documents.
March
1996 Dr. Smith requests cooperation with investigation by MAMC Inspector
General LTC Collins.
April
1996 Dr Smith returns to medical practice.
Oct
1996 Dr Smith reports violation of Whistleblower Protection to Department of
Defense Inspector General with assistance of then MAMC Inspector General LTC
Darrell Stafford.
Nov
1996 Baby V is allowed to die by the LARMC Ethics Committee with mild
meningomyelocele. The Ethics Committee may have been given incomplete
information.
Nov
1996 Joint Commission Inspection returns to Landstuhl. Is not reportedly
informed of the Baby V death, continues to be unaware of sentinel cases
unreported, as well as reprisals to Landstuhl physicians, including to those
who reported problems previously to Joint Commission Physician inspector Bert
Hurowitz, MD.
Feb
1997 Department of the Army Inspector General investigation begins.
March
1997 Dr Smith takes psychometric test; examiner Gordy Winslow tells Dr Smith
that the test was within normal limits; Psychologist Brad Powell writes summary
of psychometric test in the presence of Dr Smith and places his clinic record
in the clinic chart. Details of the complaint against BG Kevin Kiley is
contained in the written report. (Brigadier General Mack Hill, responding to a
Freedom of Information Act request, says that the document never existed, and
names the Army Surgeon General as the Denial Authority. (Read Dr. Hickey’s
letter)
April 2,
1997 OFFICIAL NOTIFICATION TO MADIGAN BY MEDCOM THAT DR. SMITH IS A
WHISTLEBLOWER
Madigan
Public Affairs Director Mike Meines (husband of Carole Meines who is custodian
of Dr Smith's Credential's file) informs Madigan Commander BG Brown by the
forwarded memorandum of Ms Cynthia Vaughn of MEDCOM, that Dr Smith is a
whistleblower with complaints against General Kiley, and that Army Times is
investigating, as follows:
“Author:
Michael Meines at MEDCEN1_MAMC
Date: 4/3/97 12:31 PM
Priority:
Normal
TO: COL William Cahill
TO: BG George Brown
Subject: Media Inquiry/Congressional Issue
----------Message
Contents--
“Head's
up.
Mike
----------Forward
Header----
“Subject: Media Inquiry/Congressional Issue
Author: Cynthia Vaughn at MEDCOM4_FSHTX
Date: 04/03/97 01:06 PM
“Army
Times reporter Grant Willis alerted me yesterday that he is beginning to look
into a situation that may have occurred at Landstuhl RMC, involving BG Kiley
(then a COL) and LTC Stephen Whitlock Smith. Smith is now assigned to MAMC.
“Willis
will likely be contacting the appropriate PAOs after he has obtained copies of
correspondence on this issue (13-page letter dated 26 Feb 97: from Smith to
Senators Boxer and Feinstein.
“According
to the reporter, Smith alleges the following:
Kiley
gave an order not to treat any ER patients that were not entitled to military
ER care, no matter what the medical condition, and that the staff was turning
people away who were in life-threatening positions (actually putting them back
in their cars). Smith considered this an illegal order, treated some
non-entitled patients, and as a result, there was some form of retaliation or
reprisal
“FYI:
This information has only been provided to MEDCOM SJA, MEDCOM IG, and those of
you included in this correspondence.
“C.
Vaughn
MEDCOM
Public Affairs”
Note:
One of the MAMC Command personnel who obtained this memorandum said the
following words to Dr. Smith: “LTC
SMITH, WATCH YOUR BACK!”
April
16 1997 the Credentials Committee routinely renews Dr Smith’s credentials. However, Brigadier General George Brown does
not sign the credentials renewal per routine.
April
17 1997 CREDENTIALS REPRISAL AGAINST THE IDENTIFIED WHISTLEBLOWER BEGINS
Suddenly,
Nancy Greenfield, RN, Madigan Joint Commission and Quality Management Director,
calls an emergency “ad hoc” credentials meeting to reduce Dr Smith's
credentials, presents psychometric test
as "abnormal." Discrepancy ensues in the credentials minutes whether
these actions by Ms Greenfield are in conformity with JCAHO requirements. Dr
Smith’s credentials are placed “under supervision.”
Sept
1997 Dr. Smith continues to insist on investigation of wrongdoing and alleged
JCAHO violations at Landstuhl. LTG Blanck orders Dr Smith to travel to MEDCOM
San Antonio; Dr Smith reports Joint Commission violations at Landstuhl as
"reckless endangerment" of patients by COL Lipsi and LTC Gillingham
who claimed that they were following explicit orders by then COL (Promotable)
Kevin Kiley, the Commander.
Oct
1997 LTG Blanck's Quality Management Directorate recommends urgent
investigation of Landstuhl.
Jan
1998 LTG Blanck belatedly accepts the decision of his Quality Management
Directorate to investigate BG Kiley’s management of Landstuhl. Only the
officers below the rgrade of General Officer are to investigated first.
June
20 1998 Ms Kelly Theriot, MAMC
Medical Claims attorney wins $500,000 settlement from MAMC.
Aug
1998 General Kussman of European Regional Command receives direction by
Department of the Army and MEDCOM to investigate Landstuhl. Dr. Smith notifies
both MAJ Richard Jordan and COL Lester Reed of Department of Medicine by
memorandum that the Landstuhl investigations are beginning to escalate and may
affect his ability to concentrate fully on his work. (The memorandum consisted
of the McClatchy Letter to the Editor plus
signed witness statements.)
Sept
1, 1998 BG Hill allegedly instigates angry confrontation with Dr Smith, after
Dr Smith had chatted with Dr Sue Bailey at a public receiving line; Mr. James
Cleaver pushes Dr Smith into an elevator, interrogates him in the Provost
Marshall's Office, accused him of carriying a concealed weapon, and pushes him
down an escalator, and orders him not to approach Dr Bailey again by order of
the MAMC Command.
Sept
6 and 10, 1998 Dr. Smith reports officially to his Department via Ms Earnestine
Russell and Ms Donna Hewitt that he is delinquent in records and requires extra
administrative time in order to bring them into compliance. He reports the
harassment of September 1 which precipitated the difficulty in concentrating on
record keeping to Provost Marshall MAJ Murphy and to Department of Medicine.
Sept
1998 Dr. Smith reports these harassment actions, and reports his consequent
difficulty in concentrating on record keeping to his assigned MAMC psychiatrist
COL Russell Hicks (on 2 occasions) and to his private physician. Dr Hicks
expresses fear in reporting the events, makes no mention in his official
evaluations of Dr. Smith for the Impaired Provider Committee for September,
October, and November. Dr. Hicks is specifically excluded from participation in
the credentials hearing of 3 March, by order of LTC Pearson, Fort Lewis JAG
Legal Officer presiding: LTC Pearson says that he is directed to say that Dr
Hicks is NOT Dr. Smith’s psychiatrist under the Impaired Provider Program.
October
9, 1998 Dr Smith reports BG Mack Hill's actions of 1 Sept 1998 as reprisal in
violation of whistleblower protection. (Read the official report made to Criminal
Investigation Division at Fort Lewis.)
October
1998 A Medical Service Corps Lieutenant, apparently not at the direction of the
Department Chief, directs assignment of the large number telephone triage
patients (over 300); assigns some directly to appointments, some with Dr.
Smith. Nursing staff complain, and an RN Maria Turner is allowed to take charge
of telephone triage under the Department Chief’s authority. Meanwhile, correspondence with both DA
IG and with COL Joseph Smith of
Heidelberg consume large amounts of Dr. Smith’s time to prepare testimony.
October
1998 Department Chief COL Les Reed and RN Maria Turner and SPC Jones “rescue”
Dr. Smith from increasing depressive symptoms by assigning him more assistance
with record keeping and patient flow under COL Reed’s direction. (See
Supervisory Plan #1)
Nov
2, 1998 Allegedly, COL Howard Cushner, not Dr Smith's supervisor, meets with
Nancy Greenfield, RN, under Command direction, in order to remove Dr Smith's
credentials, while Dr. Smith is assigned out of town for LTG Blanck’s
Telemedicine Conference in San Antonio. COL Reed, the Department Chief, is not
consulted in this action. There is no mention of Supervisory Plan #1, and why
it was being abandoned.
Nov
6 1998 COL Cushner allegedly allows announcement at clinic meeting that
"Dr Smith will not be returning, because of credentials problems."
Nov
9 1998 Dr Smith returns from San Antonio. COL Cushner orders Dr Smith not to
see any patients indefinitely, orders him to move all of his possessions out of
his office, orders him in writing to report to GS4 clerk Elizabeth Henderson as
his supervisor.
Nov
1998 As part of the investigation which MEDCOM authorized, Dr. Smith received
an alarming report originating from 2 medical personnel currently assigned to
Landstuhl. In November of 1998, they reported incomplete maintenance records
for 10 years previously on instrumentation used by LARMC Ethics Committee for
brain death determinations. The inability to predict the baseline readings
implied that it is possible to declare a person brain-dead when that person is
alive. This was reported to the investigator in Heidelberg.
Nov
20, 1998 LTC Johnston, orthopedist, diagnoses Dr Smith as having paranoid
delusions. Dr. Russell Hicks, Dr. Smith’s assigned Army psychiatrist, appears
to disassociate himself from this controversy. Nancy Greenfield maintains LTC
Johnstone's memo in Dr Smith's credentials file. Army Times later reports the
incident.
Nov
1998 COL Joseph Smith from Heidelberg, under orders of Brigadier General
Kussman, arranges a secret visit to MAMC, requests LTC Smith prepare witness
list.
Dec
2 1998 BG Mack Hill, not himself a physician, summarily suspends Dr Smith's
credentials to practice medicine.
Dec
4, 1998 Dr Peter Nielsen, close associate of BG Kiley's and key witness for the
Landstuhl investigation, reports by memo Dr Smith's involvement in the secret
investigation to BG Mack Hill's legal officer. Ms Greenfield maintains the memo
in Dr Smith's credentials records.
Dec
6, 1998 COL Smith arrives from Heidelberg. Key witnesses become suddenly
unavailable.
Dec
15, 1998 LTG Crocker assigns MAJ Cusker as Dr Smith's lawyer to file charges
against BG Mack Hill, including Article 138 of the Uniform Code of Military
Justice. The charges to be included: harassment in violation of whistleblower
protection on the day of Dr Sue Bailey's visit and Dr Smith's reported
detention and assault by MAMC security guard, and credentials reprisal.
Feb
4, 1999 BG Hill requisitions MAJ Cusker as HIS own lawyer. COL Woodling, LTG
Crocker's JAG attorney, justifies the sudden change by memorandum.
February
8, 1999 Ms Greenfield, RN, threatens punitive action against Dr Smith if Dr
Smith allows his witnesses or outside agencies to see credentials documents
under Ms Greenfield's purview. Ms Greenfield has Acting Commander COL Bauman
sign the memorandum and has CPT Geib, MAMC Medical Claims Attorney, read Dr
Smith his rights regarding the punitive action. COL Woodling, LTG Crocker's JAG
Attorney writes a memorandum to Dr Smith justifying Ms Greenfield's actions. Dr
Smith ceases preparing witnesses for fear of precipitating reprisals against
his witnesses also.
February
15, 1999 (approximately) Incoming MAMC Deputy Commander COL Gilman reportedly
arrives at Madigan for several days of briefings with COL Casey Jones and
others. Gilman reportedly obtains detailed information about the case of Dr.
Smith. Also, reportedly Gilman receives a briefing from another whistle-blower
who allegedly refused unlawful and unsafe orders to cut corners during a
nuclear cleanup at a previous assignment. The whistle-blower reportedly tells
COL Gilman that he is under reprisal by Brigadier General Mack Hill’s command.
COL Gilman replies that he (Gilman) is on a fast track toward becoming a
general officer, and therefore cannot assist the whistle-blower. Denied
assistance by the new Deputy Commander COL Gilman, the whistle-blower then
files retirement papers.
March
3, 1999 Credentials Committee votes to restore Dr Smith's credentials. As
summarized in the credentials minutes of 3 March, Nancy Greenfield, RN, refuses
to correct numerous false data and memoranda contained in Dr Smith's
credentials records. LTG Crocker's JAG officer LTC Pearson officiates at the
meeting, but does not sign the minutes.
March
22, 1999 Credentials minutes are not transcribed until now; language
recommending investigation of Dr Smith for "conduct unbecoming" and
"unprofessional conduct" is inserted into the credentials record.
Attendees at the 3 March hearing do not remember such language being present.
BG Hill signs the hearing record. The record is forwarded to MEDCOM under
control of BG Kevin Kiley, without opportunity of local appeal being afforded
to Dr Smith. Local appeal is guaranteed under Army Regulation 40-68.
April
8, 1999 Dr Smith signs the memo of understanding, restoring credentials via Dr
Patrick Kelly, Acting Deputy Commander.
May
10, 1999 University of Washington medical evaluation recommends Dr Smith be
returned to duty.
May
13, 1999 LTG Blanck agrees to accept Dr Smith's appeal and request for
retirement through mediation by COL Sid Atkinson, of MEDCOM’s Quality Management
Directorate
May
14, 1999 Dr Smith informs COL Gilman, new MAMC Deputy Commander, of Dr Smith's
desperate family and financial crisis, based on the prolonged legal expenses in
excess of $20,000.
May
25, 1999 Dr Smith sends request for retirement and full credentials to LTG
Blanck.
June
16, 1999 BG Hill per memorandum signed by new Deputy Commander COL Gilman
orders a new obstacle to Dr Smith's returning to patient care: still another
meeting requiring a lawyer, or alternatively, a tape-recorded reconvening of a
credentials hearing. COL Gilman reports to the new Troop Commander LTC Turner
that Dr Smith "is not being cooperative." COL Gilman’s memorandum
does not mention Dr. Smith’s appeal to him of 14 May for restoration of
credentials because of the numerous due process violation reported, and the
desperate financial situation precluding bringing legal counsel to more
hearings.
June
18, 1999 Dr Smith protests the new obstacle and delay. Repeats request in
writing for immediate retirement and clean credentials.
June
22, 1999 Dr Smith forwards formal appeal of credential actions to LTG Blanck,
with oversight of Dr Sue Bailey's office. Appeal of credentials actions was
based upon reported numerous departures from JCAHO standards of due process;
and refusal by Nancy Greenfield, RN, and Brigadier General Mack Hill to remove
false data from Dr Smith's credentials file.
June
1999 Dr. Smith’s financial and family situation deteriorates. He separates
temporarily from family under medical direction from his physicians. He is
ordered by Dr. Hickey to rest 3 days in order to catch up on lost sleep; Dr.
Smith reports to MAMC Emergency Room, is medicated for sleep, and is taken by
ambulance to temporary barracks on Fort Lewis, as documented in the Emergency
Room documents. Nevertheless, MAMC Command begins an investigation against him
for not reporting to duty. (Absent Without Leave). Dr Smith is also notified
belately that he had failed the Army PT Test which he had taken in April.
Exactly why the test taken in April was judged a failure in June was not fully
explained.
July
7 1999 Dr. Smith gives his retirement request to Ms Sharon Dahl, secretary to
COL Gilman. The request does not reach Fort Lewis Retirement Office (one mile
away from MAMC) until July 29.
July
12 1999 Army Times article (#2) by Karen Jowers is published, reporting the
continuing delay by BG Hill in restoring Dr. Smith’s credentials, as voted by
the 3 March credentials hearing.
July
16 1999 BG Mack Hill suddenly restores Dr Smith’s credentials “under
supervision.” COL Gilman orders the plan to begin on Monday 19 July, before Dr.
Smith’s living situation away from family is stabilized and during a week in
which Dr. Smith’s Chief Dr. Reed is assigned to be on call for the in-patient
service of students, interns, and residents.
August
13, 1999 Dr. Smith passes Army retirement physical exam at Madigan Consolidated
Troop Medical Clinic.
August
16, 1999 Dr Smith appeals directly to LTC Kaleen Curtis, Deputy, Career
Activities, to expedite retirement and credentials to make up for delays and
obstacles placed by BG Hill.
Sep
1999 Dr. Smith accepts Army Emergency Relief loan of $1900, and uses all
available leave in order to stabilize family and financial emergency. COL
Gilman refuses to extend Dr. Smith advanced leave for the purpose of retirement
and family emergency.
October 5 1999 COL Gilman takes over micro-management of
“supervisory plan”; gives adverse evaluation to Dr Smith which the designated
supervisors COL Reed and LTC Root had not given to Dr. Smith, excludes COL Reed
the Department Chief from meeting, schedules meeting to conflict with
Department of Medicine meeting when Dr Smith is scheduled to present his
informatics project to the Department, tells Dr Smith that emergency loans are not
approved per Troop Commander LTC Steve Turner, that nothing more could be done
to secure the loans. However, later review shows that loan application #2 for
Army Emergency Relief had never reached the AER office.
October
14 1999 Dr. Smith receives second Army Emergency Relief loan after Troop
Commander LTC Steve Turner signs verification of need. This was the application
which COL Gilman said had been disapproved on 4 October, but which in fact had
never reached the AER office until Dr. Smith hand carried a copy on October 13.
LTC Turner expresses surprise that his name was used by COL Gilman as verifying
the inability of AER to give the loan, and is very helpful in signing the
verification of need as required by the AER office. LTC Turner expresses concern
that LTC Smith was forced by worsening financial circumstances to move out of
the Fort Lewis Guest House (Lodge) and demonstrates willingness to explore all
housing options. Dr. Smith has a full patient care day on Thursday, but LTC
Turner agrees to call back after 1530 on Friday to discuss housing.
October
15 1999 There is still no official explanation for the “limbo” status of Dr.
Smith’s retirement request which had been hand carried to Ms Sharon Dahl, COL
Gilman’s secretary on 7 July, the same date that it had originated.
October
15 1999 1530 to 1600 hours: Dr. Smith in counseling session with his supervisor
COL Crowe continues to receive favorable reviews on documentation of medical
charts. There is no mention of any of the adverse feedback which COL Gilman had
earlier cited (5 October.)
October
18 1999 Dr Smith, accompanied by his attorney Mr. Ivan Johnson meets with COL
Peterson, I Corps and Fort Lewis Inspector General at 1145 hours. COL Peterson
accepts computer disk of protected communication for delivery to DOD IG. COL
Peterson declines to accompany Dr Smith to see the JCAHO surveyor, explaining
that the presence of Dr.Smith’s attorney is sufficient. Dr. Charles Blewett
accepts the computer disk with Dr. Smith’s protected communication to JCAHO,
documentation of alleged due process violations by Madigan Commander Brigadier
General Mack Hill, and a 30 minute discussion ensued, before interruption by
MAMC personnel. Dr. Blewett agreed to read the case and discuss this with JCAHO
for a decision on the matter.
October
26 1999 Dr Smith receives favorable written evaluations from Department Chief
COL Les Reed. There is no documentation to support the unfavorable reviews
mentioned by COL Gilman, representing BG Hill, on October 4. There is still no news
on the retirement request now pending since July 7 1999.
November
2, 1999 COL Gilman fields questions from 2 journalists regarding Dr Smith’s
case: Ed Offley of the Seattle Post-Intelligencer and Larry Miller of The
Olympian. Ms Nancy Greenfield suddenly resigns.
November
10, 1999 COL Gilman advances Dr. Smith’s re-credentialing and notifies him that
the retirement is being arranged to coincide with full recredentialing; that
this is a “precedent-setting action.”
December
7, 1999 Dr. Smith requests that Secretary of the Army Louis Caldera expunge the
false and misleading information in the credentials records, and reports to the
Secretary the stolen Madigan medical records pertaining to the case.
December
16, 1999 COL Gilman is notified by Ed Offley of the imminent publication of the
Seattle Post-Intelligencer article, and calls Dr. Smith to an emergency
meeting. COL Gilman says the retirement is denied, that Dr. Smith will have to
be medically separated from the Army, that Dr. Smith must move out of his
current office in the Adult Primary Care Clinic. The angry meeting is
documented by tape recording by Dr. Smith, as agreed on previously by the
participants.
December
17, 1999 Ed Offley of Seattle POST-INTELLIGENCER publishes a front page article
about the case: “An
Army whistle-blower's private war”
December
30, 1999 John Simpson’s article of the case appears on the front page of the
Fort Lewis RANGER: “Dr.
Smith’s War: Madigan Physician Alleges Reprisals for Whistle-blowing” COL
Gilman tells the RANGER that he did not know about the case of Dr. Smith before
May 1999, in contrast to what was reported about his (Gilman’s) trip to Madigan
on or about February 15, 1999.
January
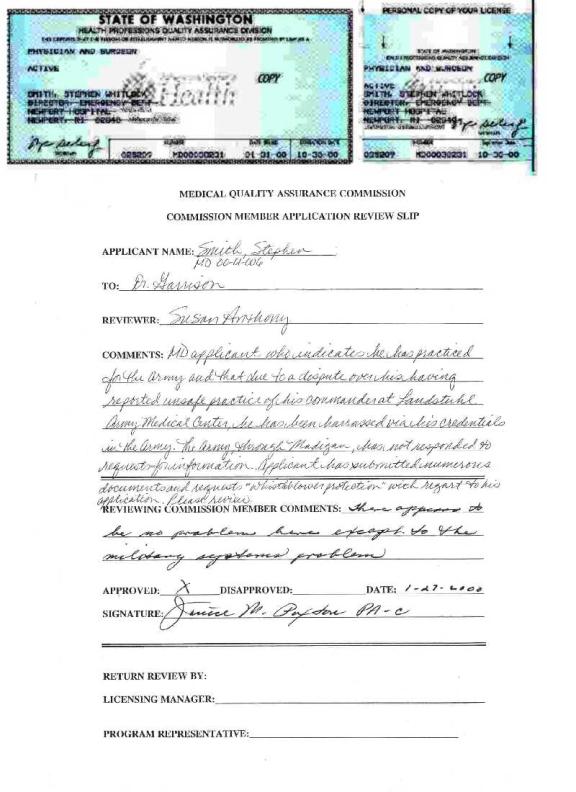
27, 2000 Washington
State Medical Quality
Assurance Commission grants Dr. Smith a full medical license under
whistle-blower protection provisions of state law. The Commission does not require
Brigadier General Mack Hill’s signature. Hill continues to refuse
to answer the letters from Quality Assurance Commission about Dr. Smith.
January 27, 2000 COL Gilman requests by
memorandum that Dr. Smith end the “90-day supervisory plan” (which has
lasted almost 11 months) so that he (Gilman) can appear to be “helping” Dr.
Smith. COL Gilman sends a correction the
next day of a serious error in the key sentence; however, no document suitable
for final signature ever follows that correction. The memo promises to shorten
the “90-day plan” by 30 days; however, 20 days of that time have already
passed. Gilman’s motivation may be to cast himself as the “good guy” and the
Credentials Committee as villain.
February 9, 2000 Dr. Smith ignores COL Gilman and
appeals directly to the Members of the Madigan Credentials to restore his
full credentials.
February 10, 2000 COL Gilman answers Dr. Smith’s
letter to the Committee, and promises restoration of credentials; however, he mentions a “special” credentials
meeting.
An Army whistle-blower's private war
Friday, December 17, 1999
By ED OFFLEY ![]()
SEATTLE POST-INTELLIGENCER MILITARY REPORTER
When Army Dr. Stephen Whitlock Smith
took over the emergency room at the Landstuhl Regional Medical Center in
Germany six years ago, he found a facility in deep crisis. The U.S. military hospital's emergency room
was suffering from acute staff shortages, aging equipment and inadequate supplies
-- so much so that Smith feared for the safety of patients and medical staff
alike. "It was the scariest
professional experience that any of us had ever thought we'd be involved
in," Smith said. Smith and his
emergency room staff pleaded for more physicians and supplies. Personnel were
working up to 60 hours a week for prolonged periods. At one point, a
psychiatric nurse was assigned to the ER to monitor symptoms of suicidal
behavior among staff members as a result of work-related stresses. After two years of fruitless requests, Smith
took a harder approach: He filed an official complaint against his Army
superiors for failing to correct the problems.
This time, Smith saw immediate results.
He was fired as head of the emergency room. The hospital commander
revoked his medical credentials. Smith was shipped 7,000 miles from his family
to Madigan Army Medical Center at Fort Lewis, where he was held in a
psychiatric ward for three weeks without a hearing. Today, three years later, the 54-year-old lieutenant colonel
remains at Fort Lewis, still engaged in guerrilla warfare with the brass, still
working in the uncertain twilight of a military medical career gone sour. And
still, he says, suffering illegal reprisals for his whistle-blowing. "This was done intentionally to muffle
me, destroy my career and family," said Smith, a soft-spoken but intense
man. "I think they are trying to wear me out and they don't care if my
family is destroyed in the process."
He is more than $30,000 in debt from lawyers' bills. For the past two
months, he has been living in a tent at a Fort Lewis recreational
campsite. What Smith wants now is
vindication, the opportunity to retire early from the Army, and to get a
civilian medical license in Washington state.
Army officials won't talk about Smith's accusations, citing the
privileged nature of most of the material involved, including Smith's own
medical records. An investigation into
Smith's original complaint filed with the inspector general at Landstuhl and a
review of working conditions at Landstuhl by the Army's European Medical
Command found no evidence to support his allegations, officials said. But the Pentagon acknowledges that the
Defense Department is investigating allegations of mismanagement at Landstuhl,
as well as Smith's complaints of reprisals from officials there and at
Madigan. Smith remains optimistic that
the investigation will clear his name and reputation. He sees his battle as a
war of attrition, and so far, Smith says, "I have survived."
An
emergency room in crisis
Smith
reported to the Landstuhl Regional Medical Center as chief of emergency medical
services in July 1993. It was his third stint as the head of an ER facility. He
had the same job at a civilian hospital in Rhode Island, then was ER chief at
an Army hospital in Denver before the transfer to Germany. Smith and his family were excited about
moving to Landstuhl. "We enjoyed
it for the day trips and weekend tours," Smith recalled. "It's the
very best part of Europe to go touring from because everything is so close,
whether France or the Bavarian Alps or the rest of Germany." But work quickly began to crowd out family
life, Smith said. The medical facility
in southwest Germany is the trauma center for all U.S. military forces in Europe,
including troops deployed to crisis areas such as Somalia, Bosnia and Kosovo.
It is open 24 hours a day, seven days a week.
Under Army policies, Smith's emergency room was supposed to have at
least seven full-time certified ER physicians. But during the summer of his
arrival at Landstuhl, the number dropped to four when departing physicians were
not replaced. In May 1994, Lt. Col.
David Gillingham arrived at Landstuhl as the new chief of ambulatory care and
Smith's immediate superior. "I
thought we would get along fine," said Smith, who was assigned to be
Gillingham's sponsor to help with his processing and moving needs. "I
picked him up at the airport and introduced him to the community." The cordiality vanished about a week
later. Smith said Gillingham rejected
his request for additional ER staffing even after being told the physicians
were being forced to work 50-60 hours per week, and Smith was forced to work
60-70 hours a week to cover both ER shifts and his administrative duties. At a meeting to discuss the ER staffing
shortage, Gillingham's reaction stunned and angered Smith. "Gillingham presided over the meeting
and ordered me 'to work the ER doctors into the ground,'" Smith said. He
quoted Gillingham as saying of the young doctors, "They are cannon fodder
and have to pay back (for) their training." The stress took a toll on
everyone working in the emergency room, including Smith. "I was marooned at work," Smith
said. "My family had to go on tours alone." Smith, who has battled clinical depression for most of his life,
said at one point he was hospitalized for nervous exhaustion. "I don't dispute the fact that I became
depressed as a result of the situation," he said. In July that year, the number of available
ER physicians dropped from four to three after a junior physician suffered a
nervous breakdown, Smith said. Landstuhl officials eased the crisis by rotating
other doctors into the ER for several months.
Smith's senior non-commissioned officer at Landstuhl, now-retired Sgt.
1st Class Stanley Gaines, said in an interview that hospital commanders refused
to take steps to find qualified physicians for the emergency room. He also said
they attempted to pressure doctors to minimize medical care to non-military
patients. "We didn't have the
amount of staff to adequately take care of our patients," said Gaines, who
now lives in Tyler, Texas. "I don't know the real reason, but we weren't
getting supported and people didn't care." By mid-1994, Landstuhl was treating more than 23,000 emergency
cases a year -- an average of 63 per day -- but receiving administrative credit
for less than half that number, Smith said.
Smith has accused Gillingham, his supervisor who also ran the hospital's
family clinic, of diverting budget money and staffing positions from the
emergency room by falsely claiming that more than 11,000 of the ER cases had
actually been treated at the family clinic. Smith said this enabled Gillingham
to obtain money and staffing support his facility otherwise would not have
received. "They were weak leaders
and in a bad situation (with overall budget cuts)," Smith said of his
bosses. "They didn't mind endangering patients to advance their
careers." That winter, Smith tried
repeatedly to obtain support from his commanders to prevent another ER staffing
crisis in the summer months when many physicians on temporary assignment to
Landstuhl normally returned to their home bases. Smith said he was promised in
February 1995 that the number of certified ER physicians would be kept at a minimum
of five -- still two below the Army minimum of seven.
Confrontation
In
May and June 1995, two events occurred at Landstuhl that set Smith on a course
of confrontation with his senior officers.
On May 8, Smith reported that the beeper system for contacting on-call
ER doctors had failed the day before at a time the emergency room experienced
several major trauma cases. "We
couldn't call in the specialists we needed to save lives," Smith said.
"In the spring, Germany is a beautiful place, and the specialists are
going to be out . . . depending on their beepers if there is an
emergency." Smith requested an
immediate replacement of the system. It didn't happen. Instead, his superiors became angry with him
for pressing the issue, Smith said.
Less than a month later, while on duty as an ER physician, Gillingham
treated a 17-year-old civilian, the son of an Army contract employee, who had
suffered a head injury, Smith said.
Smith and Gaines say Gillingham sent the boy home with a written
diagnosis of abrasions even though the youth had sustained prolonged loss of
consciousness, had a severe headache and had no memory of the event. The next day, the youth was rushed back to
Smith's emergency room in a coma. Smith
says the emergency room beeper system failed again and the on-call neurosurgeon
could not be located. In desperation, staff members rushed the unconscious
patient to another medical facility about 50 miles away for emergency brain
surgery. The youth suffered permanent
brain damage as a result of the incident, according to the Hilton Head Island,
S.C., Packet, the newspaper in the young man's hometown. According to the newspaper, the boy's family
last year filed a $7.5 million claim against the Army, alleging malpractice.
The Army judge advocate general's office ruled the hospital had not acted
improperly. The Army has final review of claims filed against the service's
overseas facilities. After the office
of Sen. Strom Thurmond, R-S.C., intervened, the family was offered a
settlement, a spokeswoman for Thurmond said. Details of the settlement were not
released. Back in Germany, things
continued to get worse for Smith and his emergency room staff. In September
1995, NATO carried out a fierce air campaign in Bosnia that paved the way for
the deployment of 40,000 U.S. and NATO troops into Bosnia. Landstuhl was
earmarked to handle any seriously injured peacekeepers. In a memo to one of his
supervisors, Col. Kevin Kiley, Smith said U.S. casualties would overwhelm his
emergency room. The dispute between
Smith and his staff on one side, and higher-ups at Landstuhl on the other,
continued to simmer. On Feb. 12, 1996, Smith formally submitted his complaint
to the inspector general at Landstuhl accusing Kiley of tolerating violations
of standards established by the Joint Commission on Accreditation of Healthcare
Organizations. The independent commission evaluates both civilian and military
hospitals for correct standards of practice and administration. Smith alleged hospital officials were
endangering patients by purposely understaffing the emergency room and that his
requests for additional doctors were repeatedly ignored. Two hours later, Kiley stripped Smith of his
medical credentials and ordered his immediate transfer to Madigan. Smith said
different officials at Landstuhl told him different things. At first, he
believed he would remain at Madigan for a brief medical checkup before
returning to Germany. Other Landstuhl officials indicated Kiley had ordered a
permanent transfer. "The paperwork
was pretty confusing, as well," Smith said. One assistant to Smith said the transfer was a reprisal. "It was done very viciously," said
Gaines, the senior sergeant in Smith's emergency room. "He (Smith) wasn't
being supported by his superiors and made some calls they didn't like, so they
struck out at him instead of solving the problem." Smith packed his bags.
Incarcerated
at Madigan
Twelve
days after the confrontation with Kiley, Smith arrived for duty at Madigan on
Feb. 24, 1996, and to his shock was locked up in the hospital psychiatric
wing. "They handed me the pajamas
that patients wear who are not allowed out, and they told me I had to hand over
all of my possessions except for my uniform," Smith recounted. "I was
stunned." He has records from his
trip that indicate he stopped at Army Medical Command offices in Washington,
D.C., en route to Madigan, where he met with officials and conducted routine
business. He said there was no indication on his travel orders that he was to
be placed under medical supervision or constraint. Smith was released from the Madigan psychiatric unit in three
weeks, and was surprised when Madigan's ER director invited him to join the ER
staff. He had his medical credentials restored in full after several weeks.
"It was as if the whole episode had not even happened," Smith
said. Smith said the incarceration
violated numerous Army regulations because there was neither a formal hearing
or any written orders committing him to the secure ward. He believes Kiley made
a telephone call to Madigan officials that led to his incarceration. Madigan officials declined comment on any
specifics of Smith's complaints, including the hospitalization, but insisted
that no patients are locked up without due process. "We don't confine people in a hospital as a rule," said
Col. Jim Gilman, Madigan's chief of medical staff and Smith's current
superior. But when Smith continued in
the following months to press for Army and Pentagon investigations into Landstuhl,
he said, officials at the Pierce County facility began engaging in reprisals
against him. In 1997, Smith said his
medical credentials were restricted again for a brief time after officials
learned the independent newspaper Army Times was investigating his case. And in
September 1998, during a visit to Madigan by Dr. Sue Bailey, assistant
secretary of defense for health affairs, Smith said he was forcibly detained by
a security guard and dragged out of the area when he approached Bailey, an
acquaintance from medical school. Smith
filed a criminal complaint with the Fort Lewis criminal investigative
detachment as a result of the dragging incident. Several weeks later, he said,
Maj. Gen. Mack Hill, commander of Madigan Army Medical Center, again restricted
his medical practice rights. Hill, like other Army officials, declined to
comment. Smith said this complaint has
been in limbo for more than a year. In March, the credentials committee at
Madigan voted to restore his authority to practice medicine. He is currently
fully active in the hospital's adult primary care clinic.
The
price of whistle-blowing
Married with two sons, one of whom still lives at home,
Smith said the stresses of the past year had become so great that he took his
family therapist's suggestion and temporarily moved out of his home. "We
decided to separate until the stress of this business was less," Smith
said. "I'm trying to protect her from all of this," he said of his
wife, Virginia. Deeply in debt from
legal expenses, Smith said the only temporary housing he could afford was a
tent staked at a campsite at North Fort Lewis, where Smith goes every day at
the end of his medical shift at Madigan.
Smith said he finally decided to request early retirement from the Army
but his application remains bogged down in the bureaucracy. Smith also is at
the mercy of Madigan officials -- the same officials whom he said have engaged
in reprisals against him -- to complete the routine paperwork that would allow
him to apply for his state medical license.
Smith remains in what he calls "suspended animation," waiting
for the Army to respond to his retirement request. He wants to get on with his
life and work as an emergency room doctor in the civilian community. Smith looks forward to rejoining his family.
He visits them on weekends. Two of the
three Army officials Smith accuses of improper actions at Landstuhl remain on
active duty. Kiley, the former
Landstuhl commander, is a two-star general serving as assistant Army surgeon
general and deputy chief of staff for force projection. He supervises all Army
physicians. Kiley declined a request to be interviewed. An Army Medical Command spokeswoman said
Kiley has recused himself from any personnel decisions involving Smith.
"He has declined to comment on this issue," said spokeswoman Cynthia
Vaughan. Gillingham, Smith's direct
superior at Landstuhl, is now a student at the U.S. Army War College in
Carlisle, Pa. He also declined comment on Smith's allegations. Lipsi, the former deputy commander for
clinical support at Landstuhl, has retired from the Army and could not be
located for comment. P-I reporter Ed
Offley can be reached at 206-448-8179 or edoffley@seattle-pi.com
Dr. Smith’s War: Madigan Physician Alleges Reprisals
for Whistle-blowing
J. M. Simpson of the FORT LEWIS RANGER December 30, 1999
In February of 1996, Dr. Stephen Smith became a
whistleblower; As a result, his life has changed.
An intense man with an affection for technology,
Smith was assigned to the emergency room at Landstuhl Regional Medical Center,
Germany. While there, the lieutenant colonel complained to the inspector
general that his superior, COL Kevin Kiley, tolerated the violation of
standards established by the Joint Commission on Accreditation of Healthcare
Organizations. The commission is an independent body that evaluates civilian
and military hospitals for correct standards of practice and administration.
Smith complained that hospital officials were
deliberately understaffing the emergency room, ignoring his requests for more
doctors, and thereby endangering both the staff and patients.
"I filed the complaint because of the lack of
due process in championing the welfare of patients and staff in Germany,"
Smith said.
Within hours of filing the complaint, Kiley stripped
Smith of his medical credentials and ordered his immediate transfer to Madigan
Army Medical Center.
When Smith arrived at Madigan on February 24, 1996,
he was locked up in the hospital's psychiatric wing. Three weeks later, he was
released and asked to join the hospital's emergency room staff.
Smith contends that his incarceration in the
psychiatric wing violated Army regulations.
He points out that there was no formal hearing and no written orders
placing him in the secure unit.
"It was all done as a cover-up for Kiley,"
Smith said. Kiley, the former Landstuhl
commander, is now a major general serving as assistant Army surgeon general and
deputy chief of staff for force projection.
In a recent interview with the Seattle
Post-Intelligencer, COL James Gilman, deputy commander for clinical services at
Madigan and Smith's current superior, was asked about Smith's incarceration.
"We don't confine people in a hospital as a rule," he said.
But when Smith continued to press Army and Pentagon
officials about his allegations concerning Landstuhl, he contends that his
superiors began to take reprisals against him.
Smith states that in March of 1997 he was
"forced" to take a psychometric test. He believes the test was used
as means to get back at him.
"MAMC command said the test results were
abnormal and that they allow it to place me under supervision," Smith
said. "I saw those scores; they are normal." Smith also went on to
say that data from his medical records is missing and that the results of the
psychometric test are part of the missing data. Smith also contends that data
from his medical files vanished only after Gilman took over as deputy commander
earlier this year.
"All of this stuff vanished when Gilman took
over," Smith stated. "Things have been in a free fall, with no one in
charge."
Madigan officials declined to comment on any aspect
about the test.
Smith says his medical credentials were renewed on
April 15, 1997, but that the following day they were revoked. On April 17 a
meeting was held; Smith was placed under the supervision of COL Les Rice, chief
of the department of medicine, and his credentials were restored.
Smith alleges that his credentials were pulled
because hospital officials learned that the independent newspaper Army Times
was investigating his whistle-blowing activities.
In December 1998, Smith said that Brigadier General
Mack Hill, MAMC commander, suspended his medical credentials. "I didn't
see any patients for eight and a half months," Smith said.
He did, however, see a psychiatrist.
On May 10, 1999, Smith was evaluated by Dr. David
Dunner, Assistant Chief of Psychiatry at the University Of Washington.
According to Smith, he does not know why he was sent to the evaluation;
however, he believes his credentials' committee, which is chaired by Gilman,
arranged the evaluation and that Hill ordered the evaluation.
Madigan officials deny that Hill and Gilman had
anything to do with the evaluation. Moreover, hospital public affairs personnel
stated that Gilman arrived at Madigan after Smith saw Dunner. Gilman, however,
arrived in April 1999.
According to Smith, it is at this point that data
from his medical records turned up missing.
"Some crucial medical records turned up
missing. They are my psychiatric clinical records, my psychology clinical
records, and my psychometric test results," Smith said.
As for the psychiatric evaluation conducted by
Dunner, Smith contends that his test results show him to be
"well-grounded."
"Dr. Smith had proven that he has done good
clinical work; that he is in remission from major clinical depression; and that
he receive his credentials and be put back to work," Smith said of
Dunner's report. "Dr. Dunner also added that Madigan might not be the best
place to stay because of the perception of reprisals," Smith added.
Smith does not deny that he has suffered from
depression. "I've been up front about it since coming to medical school on
an Army medical school scholarship," he said.
Married with two sons, one of whom lives at home,
Smith said that the stresses of the past year had become so great that he took
his family therapist’s suggestion and temporarily moved out of his home.
"I did not want to bring undue stress to my
wife," he said. Smith does, however, see family members regularly.
Smith is more than $30,000 in debt from legal bills;
he has used some of the money set aside for his children's college to pay some
costs. He allots himself $500 per month on which to live. Since he could not
afford separate housing, he has lived in a tent for the past two and a half
months at a campground on North Fort Lewis.
"What's been done to me has been to destroy me
and my family," Smith said.
Hoping to continue his career in the civilian
community, Smith requested early retirement from the Army in July 1999 and that
Madigan officials complete the paperwork that would allow him to apply for his
state medical license. In his request, Smith asked that the full restoration of
his credentials be a part of his retirement papers.
"That would be rare," said a source who
requested anonymity. "If the Army did that, it would set a precedent, and
that is unlikely to happen. But I will tell you this, there are people there
out to squash him."
Smith says his request for early retirement was
denied on December 16, 1999. Mike Meines, public affairs officer for Madigan,
says he has not seen an official denial for the retirement request.
In the meantime, Smith will witness the new
millennium in a tent on Fort Lewis, waiting for an answer.
Gilman’s memorandum to Dr. Smith requesting an end
to the “90-day plan”
COL
Gilman’s correction of the
key sentence in his memorandum
Dr. Smith’s answer to the Members of the Credentials Committee
9 February 2000
Members of the Madigan
Credentials Committee:
Thank you very much for seeing
me through the 90-day supervisory plan, the last day of which is today, as the
enclosed CHCS printout verifies. Special thanks are due to Ms. Sharon Hehn and
LTC Curtis Hobbs of the Endocrine Service who have carefully documented the
reviews of the medical charts during the full 90-day supervisory period. COL
Reed, COL Crowe, and LTC Root have been outstanding supervisors, while Ms.
Helen Pierce’s kindness knows no bounds.
Your draft letter of 27
January, as well as the edited paragraph received several days later, mentioned
the Committee’s intention to offer a waiver for the last 30 days of the plan.
Although I appreciate the Committee’s thoughtfulness in considering a waiver, most
of the 30 days of the intended waiver had already been worked under the
supervisory plan, making the waiver invitation moot. I followed wise counsel in
finishing the supervisory plan today as originally written, in order to secure
what the Committee promised me according to the top of page three of the
Supervision Plan, revised 25 March 1999:
“After 90 days of successful proctorship and supervision, privileges for
internal medicine will be recommended without supervision.”
For consideration during tomorrow’s
Credentials Committee Meeting of 10 February 2000, I respectfully request the
full Internal Medicine privileges promised by the Committee.
Sincerely,
![]()
Stephen Whitlock Smith, MD
FACP, FACEP
LTC, MC
Cc: DCCS, DCN, Chief, Department of
Anesthesia and Operative Services, Chief, Department of Emergency Medicine,
Chief, Department of Family Practice, Chief, Department of Medicine, Chief,
Department of OB/GYN, Chief, Department of Pathology, Chief, Department of
Pediatrics, Chief, Department of Psychiatry, Chief, Department of Radiology,
Chief, Department of Surgery, Chief, Physical Medicine and Rehabilitation
Service, Chief, Preventive Medicine Service, Troop Commander, Ms. Sharon Hehn,
LTC Curtis Hobbs, MAJ Burgoa, Ms. Deborah Gibson, Mr. Ivan Johnson, Mr. Mike
Gaffney
Attached: CHCS documentation
(Names and details of the patients are omitted for reasons of patient confidentiality.)
COL Gilman answers Dr. Smith’s letter to the Credentials
Committee. He mentions a “special” meeting.
---------------------------------------------------------------
"Inbox" Msg: 6 of
682
From: "Gilman, James K
COL MAMC" <James.Gilman@nw.amedd.army.mil>
To: "'Stephen
Smith'" <stevewsmith@pol.net>
Subject: RE: Fwd: Members of
the Madigan Credentials Committee
Date: 02/10/2000 05:22pm
---------------------------------------------------------------
LTC Smith:
LTC Hobbs is collating the
results of your last 30 days of charts for final presentation to the
Credentials Committee. That information was not available for today's meeting.
I hope to be able to call a special meeting next week and will do so as soon as
LTC Hobbs and COL Reed indicate that they have checked all the charts and
collated all the results. Assuming that
the last month's charts are as
good as those provided previously, I see no issues for the Credentials
Committee. However, I do need them to meet formally, hear the results of the
last month's charts, and have their actions restoring your credentials recorded
in official minutes. With regard to exactly what privileges are being restored
without supervision, I refer you to the delineation of privileges requested by
you on 28 April 1999. These are the privileges for which you have applied and
which were granted under supervision. These are the privileges which are under
consideration by the Credentials Committee.You do not have to submit any
additional charts between now and the time the Credentials Committee next
meets. Please contact me at 968-1190 if you have any questions.
COL Gilman
Dr. Smith’s new medical license from the State of Washington, issued on January 27,
2000, even without the signature of Brigadier General Mack Hill. Hill continues
to refuse to answer the letters from Quality Assurance Commission about Dr.
Smith.
DRAFT
Letter To The New Physician
20 August 1999
To the Editor, NEW PHYSICIAN:
I am grateful for the opportunity to give your
medical student and resident readership my perspective regarding my Army
Scholarship to George Washington University Medical School (MD, 1980), and my
Army residencies in Medicine (Eisenhower Army Medical Center, 1983) and
Emergency Medicine (Madigan Army Medical Center, 1987).
My training prepared me for a busy career
in both Army and civilian emergency medicine. I served in Saudi Arabia during
Desert Storm, and I felt confident of the medical centers and support personnel
wherever I practiced.
An abrupt change occurred while I was
Chief of Emergency Services under then COL Kevin Kiley, who was Commander of
Landstuhl Army Medical Center. Two of his subordinates, quoting direct orders
from COL Kiley himself, began to issue inappropriate and recklessly dangerous
orders to myself and other emergency care personnel. The orders included
abandonment of unstable patients, who could not produce ID cards,
My staff and I refused those orders as
unlawful and dangerous; we came under reprisal for our courage. There were
several very serious incidences of harm to patient. Consequently, I filed
charges against now-Brigadier General Kiley and his former subordinates. All
resultant investigations have been slow in being prosecuted, and are not
finalized.
The Medical Center to which I am currently
assigned
is Madigan Army Medical Center. Madigan is where I trained in Emergency
Medicine. Last September 1, I was attending a public ceremony for the
inauguration of Madigan's Medicare Program. I was at that time assigned to
Acute Care Internal Medicine; a large part of my practice consisted of
Medicare-age patients.
After I had had a pleasant chat with Dr
Sue Bailey, Assistant Secretary of Defense for Health Affairs, Brigadier General
Mack Hill approached me rapidly, and in apparent extreme anger. Later, a
hospital security guard approached me, pushed me into an elevator, accused me
of carrying a concealed weapon, and ordered me not to approach Dr Bailey's
group again. He then shoved me down the escalator heading toward my clinic.
I reported the incident as reprisal for my
part in the escalating investigations against Brigadier General Kiley. General
Hill is a close associate of General Kiley's, and 2 weeks after the incident became
Madigan's new Commander. He is the only non-physician ever to occupy that
position.
A staggering number of adverse
credentialing actions were then imposed upon me, in general instrumented by the
Joint Commission RN Representative of Madigan Ms Nancy Greenfield. Because
neither Army Regulation nor Joint Commission guidelines of due process in
credentialing were followed, I have been obligated to accuse Ms Greenfield of
acting under the unlawful orders of BG Hill to deny me due process in reprisal
for my whistleblower activities against General Kiley.
This has now gone on to direct appeal to
LTG Blanck, Surgeon General of the Army. It remains to be seen if there is ever
an adequate investigation of danger to patients under then COL Kiley's
leadership at Landstuhl.
I am hopeful that I will obtain both
retirement and clean credentials. However, the sad thing is that both Landstuhl
and Madigan Commanders have been so fearful of outside scrutiny of their
actions that they have stooped to utilize very obvious reprisal actions in
order to deflect any attempt to investigate.
I am aware that civilian HMO's have
similar pressures on their leadership. However, the Army places unusual degrees
of autonomy and power upon its commanders, this for faster response during
wartime.
My opinion is that until the tendency for
weak leaders who fear any investigation to overreact, even past the point of
criminal wrongdoing, is minimized by greater scrutiny and oversight, I would
not advise medical students and residents to accept any obligated time in the
Army Medical Corps.
This is sad, for the Army Medical Corps
largely contains well-trained and compassionate physicians.
Stephen Whitlock Smith, MD
***************************************************************************
Letter to
Dr Bailey, Assistant Secretary of Defense for Health Affairs
18 October 1999
RE: Freedom of Information Act Request
Dr Sue Bailey:
I am grateful for your salutary influence
upon my request to obtain due process in credentialing as provided for my Army
Regulation and Joint Commission and HCFA guidelines.
Because my appeal of the adverse
credentials actions against me at Madigan, as carried out by Ms Nancy
Greenfield on orders of BG Hill, has already gone to LTG Blanck personally, I am
asking your oversight of this process.
BG Hill has refused to provide the
majority of the critically important documents under Freedom of Information
Act. The FOIA Office at MEDCOM San Antonio has answered for BG Hill, naming the
Army Surgeon General as "denial authority."
Your role in this process proceeds from
several sources, as follows. I will therefore categorize my request for groups
of documents through your office, following the same categories corresponding
with your oversight over the total situation:
1. DOD Directive for Improper Mental
Health Referrals:
a. The Assistant Secretary of Defense for
Health Affairs is the oversight authority for Improper Mental Health Referrals
as provided for in DOD Directive....
b. Your training in Neuropsychiatry
qualifies you admirably to judge such Improper Mental Health referrals from a
medical and compassionate basis, rather than a purely administrative one.
FOIA REQUEST REGARDING IMPROPER MENTAL
HEALTH EVALUATIONS: I request a full set of documents exchanged between Madigan
Command, Landstuhl Command, and OTSG/MEDCOM corroborating that then-COL Kiley's
denial of due process to me was outside of Directive.
2. Your Neuropsychiatry training allows
your greater understanding of the allegedly substandard care given the teenage
boy with prolonged loss of consciousness on 3 June 1995, by one of then-COL
Kiley's subordinates.
FOIA REQUEST REGARDING THE JUNE 1995
BRAIN-DAMAGE CASE: I request corroboration that the family of the patient will
be given every consideration for their medical claim, irrespective of the fact
that a payment in the case would reflect poorly on then-COL Kiley's leadership.
3. The same background also allows your
professional insight into the Landstuhl Ethics Committee decision, allegedly
Command-directed by then-COL Kiley, to allow Baby Victoria to die with only
mild meningomyelocele.
FOIA REQUEST REGARDING THE UNFORTUNATE
DEATH OF BABY V: What assurance does the documentary record reveal to reassure
Army patients and their families that INFANTICIDE has no place legally in the
armamentarium of a Commander, and that it will not be condoned?
4. Your presence at the 1 September 1998
Inauguration of TriCare Senior Prime and your discussion with me, immediately
after which I reported alleged harassment by BG Hill, has allowed you to be my
best witness in my report of the incident.
FOIA REQUEST REGARDING MY REPORT OF
DETENTION AND PHYSICAL ASSAULT: What documents can you provide of BG Hill's
personal involvement in the reprisal action. Are you in receipt of BG Hill's
written memorandum explaining his own personal role in this lamentable and
shameful episode?
5. Your oversight of HCFA regulations
would allow you to recognize that Madigan is held to standards of Joint
Commission guidelines of due process in medical credentialing. Typically, Army
Medical Centers utilize Army Regulations to show compliance with JCAHO and HCFA
standards. If they do not do so, they jeopardize loss of considerable amounts
of Medicare financing.
FOIA REQUEST REGARDING ALLEGED JCAHO AND
ARMY REGULATION VIOLATIONS OF DUE PROCESS AT MAMC: My counsel and I require
documentary evidence of ANY JAG legal review of the many months of credential
actions against me. By memoranda produced by COL Dale Woodling, LTG Crocker's
JAG, he is presumed to be the officiating lawyer. However, why did the JAG
officer, also reporting to LTG Crocker, LTC Pearson, who actually was present
at the hearings, not sign even one of the hearing minutes?
Thank you,
Stephen Whitlock Smith, MD
***************************************************************************
18 October 1999
Letter to
American Association of Retired Persons AARP:
While I was Chief of Emergency Services at
Landstuhl Army Medical Center, I reported an abrupt erosion of standards of care,
especially as dispensed to dependents of retirees, as well as to children.
The main risk to dependents of retirees
appeared to be denial of care while in the midst of a medical emergency, if
they could not immediately prove eligibility.
Two subordinates of then COL Kevin Kiley
ordered myself and other emergency personnel to turn away certain patients whom
we considered at high risk of serious illness and injury if not monitored.
I reported these events so that other
patients would not be endangered, then found myself under reprisal by BG Mack
Hill for doing so. In a particularly dramatic event, after I spoke briefly to
Dr Sue Bailey, Assistant Secretary of Defense for Health Affairs (Medicare), I
reported that BG Hill personally approached me in anger; thereafter, I
experienced detention and physical assault by the hospital security guard.
The hearing, which addressed these strange
happenings, revealed that MAMC Command was worried about a violent protest by
Army retirees who had not been selected for the Medicare project. Would the
security guard have also detained and roughly handled the retirees if they had
become any kind of danger in the perspective of the Command?
I am grateful to the retired patients of
Madigan, having much accumulated wisdom from their own military careers, who
have been my local experts in how to write up and request investigation of
these events.
Thank you,
Stephen Whitlock Smith, MD
***************************************************************************
Tacoma, Washington, 18 October 1999
Dear Editor:
I am an Army doctor with board
certification in 2 specialties, Emergency Medicine and Internal Medicine. When
I was Chief of Emergency Medicine at Landstuhl Army Medical Center in 1996, I
complained in writing to my Commander, Dr Kevin Kiley, about my supervisors'
orders for emergency staff to send patients away without treatment, and about
the deteriorating beeper system and ambulance systems which were not operating
according to safe guidelines. I reported one case of brain injury in a child
who had been turned away without complete treatment. 2 hours after filing my
report, Dr Kiley ordered to be sent 7,000 miles to Madigan Army Medical Center
for psychiatric evaluation and spend 3 weeks in a locked psychiatric ward. I
returned to medical practice at Madigan Army Medical Center; however, I
continued to request full investigation, so that others would not be harmed.
Meanwhile, Dr Kiley became Brigadier General Kiley, Assistant Surgeon General
with authority over medical credentialing matters, and his close associate
Brigadier General Mack Hill was sent to be Commander of Madigan starting in
September 1998, just when the investigations of Landstuhl were due to begin. On
1 September 1998, I waited with dozens of other Madigan staff in a public,
receiving line, and chatted briefly with visiting dignitary Dr Sue Bailey who
had trained at the same medical center as I. Suddenly, Brigadier General Mack
Hill rushed toward me with his anger apparently directed toward me. A hospital
security guard approached me and pushed me into an elevator, interrogated me,
and pushed me down the escalator toward my clinic, ordering me not to
participate further in the meetings with Dr Bailey. I protested such treatment as reprisal for the Landstuhl
complaint against General Kiley. My official sworn statement was then placed
into my medical credentials file, and General Hill has refused to allow me to
practice medicine at Madigan for 8 ½ months. My appeal has gone to Army Surgeon
General Ronald Blanck. However, there has been an inordinate delay in the
progress of the appeal paperwork between San Antonio where General Kiley is in
overall charge of credentials, and Washington, DC, where General Blanck is. I
and my legal counsel believe that this is the first time that an Army trained
physician has been left without medical credentials for 8 ½ months in reprisal
for an Inspector General complaint of danger to patients. What does this mean to Madigan Army Medical
Center, which is embarking upon a new Medicare project? Will other doctors at
Madigan be under reprisal if they refuse to follow dangerously inadequate
medical standards for cost reasons?
What does this mean for Army medicine? Will doctors and nurses continue
to serve in our Army if the standards are deliberately lowered, and if there
are reprisals for requesting to stay within safe guidelines of patient
care? Army Times (Gannett) and Hilton
Head Island Packet (McClatchy) have published reports of these happenings,
which I attach to this letter. The situation is very unstable: General Hill has
continued to refuse my full restoration of credentials, and has refused to
verify my status for my Washington State license. I believe that Army patients
and especially retirees should worry if one of their doctors can be punished
for speaking out in favor of safe standards of care.
Stephen Whitlock Smith, MD
Lieutenant Colonel, US Army
FACEP, FACP
Stephen Whitlock Smith, MD
8103 Steilacoom Blvd SW PMB #28
Lakewood, WA 98498-6102
Tel 253-576-6746
E-Mail stevewsmith@pol.net
Senator Thurmond (202) 224-1300, Dr Sue
Bailey, Assistant Secretary of Defense
for Health Affairs (703) 614-3537, Gannett
(703) 558-3902, McClatchy (916)
321-1109, AARP 206-517-9350, American
Medical Student Association (703) 620-
6445
***************************************************************************
(Extract
from HILTON HEAD ISLAND PACKET, McClatchy Company)
See WWW.islandpacket.com
Header: Category: Local News, Creator:
Mike Ramsey, Paper Date: 7/28/98,
Paper Page/Section: 1A, End of Header.
BY MIKE RAMSEY Packet staff writer
Bobby Wood was an experienced off-road
cyclist, an "A" student and computer whiz when a bicycle wreck three
years ago sent him into a coma and changed his life. Wood, now 20 and living on
Hilton Head Island, still rides his bike every day and has been taking design
courses at Savannah College of Art and Design. But it¹s not the life he
planned. He suffered brain damage, as well as loss of vision and some mobility,
and he canceled his plans to attend Rochester University on a $32,000
scholarship. Worse, Wood and his family contend the damage might have been
prevented had he received proper care at a U.S. military hospital in Germany,
where Wood was living when the accident happened. "I¹m angry, but what can
I do?" Wood said. "They know they have done something wrong, but
won¹t do anything about it." Wood has filed a claim against the U.S. Army
for malpractice, but he and his family aren¹t optimistic. The Army¹s Office of
the Judge Advocate General in March turned down Wood¹s initial claim for $7.5
million. Wood¹s attorney filed an appeal and the results of the appeal should
be back in a few weeks. If the appeal is denied, Wood has no recourse, said
Pamela Brem, an attorney working for Wood. The case has attracted the attention
of U.S. Sen. Strom Thurmond, R-S.C., chairman of the Senate Armed Services
Committee. Thurmond has ordered an inquiry into whether the Army¹s review of
the case was thorough and above-board.
John De Crosta, Thurmond¹s press secretary, said it probably would take
several months before any investigation results would be available. Wood was 17
years old in June 1995 when he fell off his bike and hit his head. He knows he
was knocked unconscious, but does not know for how long. Wood's mother, Nohy
Wood, took him to the closest hospital, Landstuhl Regional Medical Center, a
military hospital. It was a holiday
weekend in Germany, and no local doctors were available, she said. Landstuhl¹s
emergency-room doctor sent Wood home after treating him for scrapes and
bruises, according to Wood¹s claim. The doctor didn¹t admit Wood for
observation or perform a CT scan. The
next day, Wood started bleeding inside his skull, cutting off oxygen to his
brain, according to the claim. When Wood¹s parents took him back to the
hospital, there was no neurosurgeon at the hospital to perform surgery. Wood
had to be taken to another hospital, delaying surgery by 70 minutes, the claim
states. He stayed in a coma for two weeks and suffered brain damage. Wood maintains that the emergency room
doctor the first day should have admitted him to the hospital for observation
and performed a CT scan. That would be standard procedure for anyone who lost consciousness
for more than 30 seconds. Legal
hurdles, i.e. Wood¹s legal battle with the Army is made even more difficult
because claims against the military are handled differently than other types of
civil claims. Brem said a division of the Army, called the Office of the
Inspector General, investigates claims against the Army. In addition, Army officers investigate and
decide the claims. If they deny a claim, a victim can appeal the decision to
federal court and go before an independent judge and jury. But if the incident
occurs overseas, the process stops with the Army. "It¹s a good faith system," Brem said.
"Potentially, the Army could come back and say, Yes, we were negligent,
but we still aren¹t going to award you damages." Another lawyer working on
Wood¹s case, Richard Weiss of Boston, said he may file a lawsuit in federal
court accusing the Army investigators of "not acting in good faith."
He said facts had been ignored or unaddressed in the Army¹s denial.
"Self-regulation doesn¹t work on any level," Brem said. "One of
the reasons doctors here work so hard to maintain high standards is the fear of
malpractice. Doctors at the (military) hospitals overseas don¹t worry because
they know people can¹t touch them." The lawsuit could end up in the U.S.
Supreme Court, Brem said. Similar lawsuits, which attack the law governing this
case have been challenged, but upheld by the Supreme Court. Dr. Stephen Smith,
the former emergency room chief who saw Wood on his second visit to the
hospital, has filed a series of complaints against the leadership at Landstuhl,
citing Wood¹s treatment as one example of a number of problems. Despite what Brem calls "extremely
substantial" evidence supporting Wood¹s claim, neither she nor Weiss are
optimistic about winning the appeal. Weiss claimed in the appeal that the Army
investigator, Maj. Douglas Dribben, "misstated or distorted facts" in
the case. Neither Dribben nor any other official in the Army Claims Service
could be reached for comment. In
turning down the claim, the Army investigators said his parents should have
brought him back to the hospital earlier, when Wood experienced shooting pain
in his head. And the denial states that a CT scan the first day would not have
revealed the bleeding in Wood¹s head because it didn¹t start until the next
day. But Smith said that wasn¹t necessarily true, and the doctor should have
held the boy overnight anyway for observation because Wood had lost
consciousness during the fall.
***************************************************************************
Extract from Army Times 19 July 1999
See www.armytimes.com
Newslines: The Army
Doc: Whistle blowing cost him medical
privileges
By Karen Jowers Times Staff Writer
A doctor has accused officials at Madigan Army
Medical Center at Fort Lewis, Wash., of withholding his medical privileges as
retribution for his whistle-blowing activities, and he is calling for an
investigation. Meanwhile, Army Lt Col Stephen Whitlock Smith, 51, has asked
permission to retire from the Army, with restoration of his medical
credentials. In March, the medical credentials committee held a hearing on
whether to restore or permanently pull Smith's medical privileges, which had
been revoked for alleged lax record keeping. He was told the committee
recommended his credentials be restored, but no action has been taken. On April
2, he agreed to a psychiatric evaluation, which he submitted to, and to resume
practicing medicine under supervision. The evaluation cleared him to work, his
credentials are still being held. Smith has asked for retirement and has been
told he can leave by Sept. 1. But that offer hasn't addressed his credentials.
'My credentials are more important to me than retirement,' he said. They affect
his livelihood, and he said he won't retire without them. Sharon Ayala, spokeswoman for Madigan, said
that, to protect the privacy of all involved, she couldn't comment on the
credentials issue. However, she said, 'All of the proper protocols were adhered
to in the case of Dr. Smith.' Smith's
problems began in February 1996 when he filed a complaint with the inspector
general at Landstuhl Army Medical Center, alleging hospital officials were
endangering patients by purposefully understaffing the emergency room. Smith,
who was chief of emergency medical services at the time, said his repeated
requests for assistance were ignored.
Eight days later, he was medically evacuated to Madigan for psychiatric
evaluation and spent three weeks in a locked psychiatric ward. He was allowed
to slowly return to medical practice at Madigan but continued to press for
investigations of Landstuhl. He believes his credentials problem began after
the Army launched a probe in 1998 and is the result of close ties between some
Madigan doctors and the former Landstuhl officials mentioned in his
allegations. Smith was told his credentials were pulled because he had not kept
his records up to date. In an earlier interview with the Army Times, Smith's
psychiatrist, Dr. Deborah Hickey, said she believed Madigan officials
overreacted. 'The information was there, but just not in the format they
wanted,' she said. There was no reason to believe Smith couldn't function fully
as a physician, she said. Smith has asked for investigations of Madigan by the
Army surgeon general, the assistant secretary of defense for health affairs,
the Defense Department
inspector general, and a national
organization responsible for accreditation of
military hospitals.
***************************************************************************
Extract, Army Times 15 Feb 1999
www.armytimes.com
Newslines-The Army
Fit for duty?
Army says he's mentally ill: doctor, a whistleblower, says it's a case of
retribution
By Karen Jowers Times Staff Writer
Lt. Col. Stephen Whitlock is living a
nightmare. An Army doctor for 15 years, he faces a hearing Feb. 10 on whether
his medical credentials should be revoked. He has been held in confinement for
psychiatric evaluation, removed forcibly from contact with top military medical
officials and branded as behaving in a 'bizarre' manner. To Smith, 51, it's a
case of retribution. He says his troubles started when he blew the whistle on
understaffing at an Army hospital in Germany two years ago. To the Army, it's a
simple matter of whether Smith is fit for duty. Officials at Madigan Army
Medical Center, Fort Lewis, Wash., aren't saying much about the case because
it's under investigation. But documents obtained by Army Times point to
allegations of inadequate record keeping and concerns that Smith may be
experiencing 'paranoid delusions.' Whichever side is right, Smith's story is a
case study of how an individual can get tangled up in a web of bureaucratic,
legal, and medical confusion that can threaten both a military career and a
future civilian one, as well. A former Army investigator describes Smith's case
as a classic example of what can happen to whistleblowers. 'They pay a heavy
price,' he said. 'They get so angry, so frustrated, so depressed. They think
it's the whole Army against them. And they're right,' said Jeff Lynch, who
retired in 1991 as a Colonel in the Medical Service Corps. In his last two
assignments, he worked as an inspector general. He has seen medical officers
thrown into psychiatric wards and face hearings to remove their credentials, he
said. Although he hasn't investigated Smith's case, he has reviewed it. 'I
don't think that Smith was on the planet if he weren't a whistleblower,' Lynch
said. He describes Smith as 'courageous and tenacious.'
From medical chief to patient
Smith's story is a long and complicated
one, beginning when he was chief of emergency medical services at Landstuhl
Regional Medical Center in Germany from July 1993 through early 1996. The joint
Army-Air Force medical facility is the only military hospital in central
Europe, with doctors and patients from all services. In February 1996 he alleged hospital officials were purposely
understaffing the emergency room, putting patients and staff at risk, despite
his repeated requests for more assistance.
That's when Smith's world began to fall apart. Eight days after filing a
formal complaint with the hospital inspector general, Smith was medically
evacuated for a psychiatric evaluation. Sent to Madigan, he spent three weeks
in a locked psychiatric ward. Then, he was allowed to slowly return to medical
practice, but at Madigan, not Landstuhl. However, he has not been allowed to
return full time to his specialty, emergency medicine. Still concerned about
his original complaint, Smith pressed on, this time with the Army inspector
general. That complaint, lodged in October 1996 is still being investigated,
Army officials say. Meanwhile, Army officials ordered an investigation by
European Regional Medical
Command officials, too. And when those
investigators began interviewing people in the case last fall, reprisals began,
Smith contends. On Nov. 9, 1998, Smith was ordered to stop seeing patients and
told to move out of his office at Madigan. He refused to leave his office, but
with his medical privileges temporarily suspended, he has ceased seeing
patients. 'This is a cover-up of events that transpired to hurt patients,'
Smith said. 'They're trying to get me out of here.'
'Paranoid' or not
Such statements play into the Army's case
that Smith has 'paranoid delusions.' But Smith's psychiatrist disagrees.
'There's no reason to believe he can't
function fully as a physician,' said Dr. Deborah Hickey, a retired Army colonel
and Smith's psychiatrist since early 1996. 'He's very logical in his thinking
and very bright.' Hickey, who was chief
of psychiatry at Madigan for two years before she retired in 1996, shoots holes
in the Army's charges, which include allegations that Smith's record keeping
was incomplete, that he did not sufficiently document his actions and
treatments on patients' records. Those allegations seem to be an overreaction,'
Hickey said. 'The information was
there, but not in the format they wanted.
'In his case, they found his records to be lacking in the format desired
and have used that to steamroll him without due process or the opportunity to
bring them up to standards,' Hickey said.
THE ARMY'S SIDE
Cynthia Vaughan, spokeswoman for the Army
Medical Command, said the Army has little to say right now, since the
investigations aren't complete. 'Some investigations are still ongoing, but in
the parts of the investigations that have been completed, there has been no
evidence of wrongdoing' by the Army, she said.
Brig. Gen. Kevin C. Kiley, commander of Landstuhl Regional Medical
Center during the time of Smith's complaint, declined to be interviewed. He is
now an assistant surgeon general.
Madigan's credentials committee began reviewing Smith's case in October,
based on allegations that he had not kept his patients' records up to date,
Smith said. He contends he keeps his
records in his computer and has been lax in transferring them to the printed
form. 'And I did get depressed and slowed down,' he said. 'Intimidation works.'
Hospital officials also expressed concern last fall about Smith's psychiatric
condition. On Nov. 20, 1998, Lt. Col.
Frederic Johnstone, Chairman of the Madigan Provider Health Program, wrote to
Smith's psychiatrist, Hickey, asking if there had been an 'acute change' in
Smith's mental status. 'I am concerned
that he may be currently experiencing paranoid delusion,' Johnstone wrote. 'I
am concerned that his underlying psychiatric condition may be more severe than
we suspected. We have had multiple reports of fairly bizarre behavior.'
Hickey didn't respond. 'I felt the whole
thing was totally irregular,' she said. 'They haven't gone by any procedure
I've seen in reviewing the competency of a health care provider.' Hickey said 'there has been no set policy or
procedure for dealing with Dr. Smith. All of the allegations have come from
those who are not professionals in the area of mental health.' Smith said there have been other incidents
that show he is the victim of reprisal. He filed a complaint alleging he was
harassed Sept. 1, during a visit to Madigan by Dr. Sue Bailey, assistant
secretary o defense for health affairs. He said he spoke to Bailey, an
ex-medical school classmate, for about 3 minutes. Shortly afterward, a Madigan
official confronted him angrily. 'There were witnesses that he ordered my
arrest after seeing me talk to Dr. Bailey,' A security officer approached him,
took him to another room, and said that he had been accused of carrying a gun,
Smith said. He then forced Smith to return to his duty area. Smith alleges that
the security officer forced him to walk to the escalator, holding his arm
behind his back. 'He pushed me down the escalator,'
Smith said. 'It's clearly not something
the security person did on his own.'
But Sharon Ayala, spokeswoman for Madigan Army Medical Center, dismissed
those claims. 'He was not arrested, not handcuffed, detained, nothing,' she
said. 'He was just escorted from the Command suite. We were ready to move (Dr
Bailey) from one briefing room to the next, and Dr. Smith was not part of the
group. He was not invited.'
'NO CONNECTION'
Ayala said there's 'no truth' to Smith's
allegations that the review of his credentials is connected to any complaints
he has filed. 'Madigan is committed to upholding the regulations against
reprisal,' Ayala said. Smith admits he has had a history of depression, dating
back to the time he was 18 years old. The Army admitted him into its medical
scholarship program with full knowledge of his medical history. His depression
grew worse at Landstuhl, he said, as a result of the grueling hours and poor
working conditions. Although he and others repeatedly asked for assistance, it
was denied, he said. Other medical professionals who worked in the emergency
room at Landstuhl support that contention.
'We were very much understaffed and were very proactive about saying
what we needed,' said one military nurse.
'We had three doctors and Steve (Smith) to work a 24-hour-a-day
schedule. 'At the end, we felt no one
would pay attention until we killed somebody...Anything we tried to do to fix
the problem, was stopped,' the nurse said. 'Steve would do anything for us. He
did his best, but in the end, it broke him. It was awful to see what they did
to him. 'I've never seen anything like
it,' she said. In late 1995, Smith's supervisors were replaced, she said, and
the emergency room was put 'on track. But why did they allow the situation to
continue for two years?' The answer to that question remains elusive, subject
to the Army's ongoing investigation. The answer to what will become of Smith,
however, should come sooner-perhaps directly after his Feb. 10 board
appearance.
(PHOTOGRAPH CAPTION:
'Dr. Stephen W. Smith blew the whistle on
understaffing at an Army hospital. Now
The Army wants to revoke his medical
credentials.’)
EXCERPTS FROM CORRESPONDENTS INCLUDING MS
JULIE APPLEBY
CURRENTLY CORRESPONDENT FOR GANNETT'S USA
TODAY
Published on October 23, 1998
Kaiser receives a surprise visit from
inspectors
Officials conduct an intensive
investigation into new complaints about the Walnut Creek hospital
By Julie Appleby TIMES STAFF WRITER
Kaiser Bargaining Alert
10/12/97
RETURN TO BARGAINING
To: Kaiser Permanente
From: California Nurses Association
Re: CNA/Kaiser Permanente Contract
Negotiations
In the best interests of our patients, our
members and all employees please immediately:
RETURN TO BARGAINING
We believe that before more damage is done
to your reputation in California and nationally that you should:
Drop Your Unnecessary, Massive Concessions
(13)
Provide RNs/N.S. A Therapeutic and
Enforceable Voice In Patient Care Join With CNA To Resolve Current Regulatory
Patient Care Issues
If you refuse because Kaiser Corp's
attention is focused on a mission of expansion and cost cutting rather than
patient care, Kaiser patients will read more of the following:
SAN FRANCISCO CHRONICLE
October 10, 1997
East Bay Kaiser Hospitals Face Loss of
Certification Health regulators say problems need to be fixed soon
By Michael Hytha, Chronicle Staff Writer
(excerpts)
Kaiser Permanente hospitals in Walnut Creek
and Martinez once again face the loss of their federal certification -- unless
they can correct problems with medical care by November 14, health regulators
warned yesterday. The new threat comes after months of bad news for Kaiser, the
country's largest nonprofit health maintenance organization. Earlier this year,
its Richmond and Oakland hospitals narrowly avoided the loss of their Medicare
certification after the deaths of patients transferred from the Richmond
emergency room. Kaiser's registered nurses, working without a contract since
January, have staged short-term strikes throughout the region and are waging a
campaign to force Kaiser to reverse a series of cost- and staff-cutting
efforts.
CONTRA COSTA TIMES
October 10, 1997
2 KAISER HOSPITALS STILL UNDER FEDS' FIRE
By Julie Appleby, Times Staff Writer
(excerpts)
Kaiser Permanente has failed to correct
some of the serious problems uncovered at its Walnut Creek and Martinez
hospitals, prompting an ultimatum from federal officials. The HMO was told
Thursday that unless it boosts nurse staffing in its intensive care units and
improves quality assurance programs by November 14, it will lose Medicare
funding at the two facilities. CNA
members voted overwhelmingly to hold a region wide one (1) day strike in late
October unless Kaiser returns to the table and resolves this dispute.
Hospitals & HMOs cut care, make record
profit & patients pay the price. If you feel your health care or that of
your loved ones has suffered,
Please write or call CNA's Patient Watch
Program: 1145 Market Street, Suite 1100 Market Street, Suite 1100, San
Francisco, CA 94103, 1-800-440-6877, email: patientwatch@igc.org
For the second time in 16 months, federal
officials have conducted a wide-ranging surprise inspection of Kaiser
Permanente's Walnut Creek Medical Center after receiving a number of
complaints, the Times has learned. The complaints included concerns over delays
in patient care, both in the emergency room and elsewhere in the hospital,
according to Gil Martinez, district manager for the state's Department of
Health Services. A team of investigators authorized by the federal Health Care
Financing Administration arrived at the hospital Oct. 6 and spent three days
looking into recent events that led to the complaints. Kaiser officials said
they cooperated fully with investigators and are optimistic that the findings
will show no serious problems. "The primary person that reviewed us said
the findings are not serious and are
Easily corrected," said Joseph
Macaluso, Kaiser's director of regulatory compliance. The problems uncovered
included occasional delays in transferring patients by ambulance to other
hospitals and in admitting patients to the hospital, Macaluso said. The
investigators' findings are being prepared for submission to the federal
agency. If the financing administration determines that serious problems exist,
Kaiser could be threatened with the loss of its Medicare funding at the
hospital. A similar funding threat was made by federal officials in June 1997
when inspectors swept into Kaiser's Walnut Creek and Martinez hospitals after
receiving complaints about patient care. The team cited the hospital for
inadequate staffing, long delays in emergency room care, unlocked drug storage
cabinets, sloppy record keeping and a quality assurance program that failed to
uncover the problems. After initially failing a follow-up inspection, the
hospitals eventually corrected the deficiencies to the federal agency's
satisfaction. The funding threat was withdrawn. This month's inspection is
related to deficiencies the state found in September when it looked into the
deaths of two patients, 7-year-old Gregory McCan of San Ramon and 37-year-old
Honorio Darauay of Walnut Creek. After reviewing those cases, state investigators
sought additional review from the federal agency for a backlog of other
complaints, Martinez said. Earlier this month, Kaiser's plan to correct the
problems brought up in the McCan case was accepted by state officials. McCan
died of a virulent blood infection after spending hours being treated and
monitored in Kaiser's emergency room and pediatric ward. Inspectors said Kaiser
violated its own protocols by taking more than an hour to have a pediatrician
assess the boy. It also had adult patients in a pediatric ward, causing a delay
in admitting the boy to that unit. Kaiser said it will make it clear to its
doctors that they must report to the emergency room within 60 minutes of being
called for a consultation. It will also never completely fill the pediatric
ward with adult patients, Macaluso said. In the Darauay case, inspectors said
Kaiser failed to pump the man's stomach, misinterpreted a blood test and failed
to admit him to an intensive care unit. Kaiser officials have disputed those
findings and are seeking a third-party review of its efforts. The man, who had
injected himself with a pesticide, died at the county's psychiatric ward after
being transferred there from Kaiser.
Edition: CCT, Section:
A, Page: 3
(c) 1998 Contra Costa Times
*****************************************************************************************
Hospital
oversight criticized System is too lenient, report says
By Julie Appleby
Wed., July 21, 1999
FINAL EDITION
Section: NEWS Page 1A
Federal investigators criticized the way
U.S. hospitals are inspected Tuesday, saying the process is too lenient and
often misses poor care. The system
responsible for ensuring safety is ''unlikely to detect substandard patterns of
care'' such as inappropriate surgery or high complication rates, their report
says. The strongly worded report from the Office of the Inspector General says
the government should require:
* More surprise inspections. Hospitals
currently have plenty of warning before inspections, which occur every three
years. They often spiff up the facilities, train staff on answering inspectors'
questions and even hold ''practice'' inspections.
* Review of randomly selected patient
records. Now hospitals handpick patient records for inspectors.
* More background information for inspectors
rather than reliance on hospitals to acknowledge major problems. Currently,
inspectors often don't have even media reports about troubles such as medical
errors, chronic understaffing or financial difficulties. ''If a hospital had something it didn't want
you to find, it could keep you from finding it,'' said George Grob, deputy
inspector general. The current
inspection program does help educe risk, the report says, but doesn't do enough
to spot problems. The inspector general spent two years investigating the
hospital oversight system, prompted by advocacy group complaints and
high-profile media reports about serious problems such as patients who had the
wrong limbs amputated. The report's findings didn't surprise critics of the
oversight system, who have been calling for changes for years. ''The question is, how many more people will
have to die before we do something?'' said Sidney Wolfe, director of the Public
Citizen Health Research Group, a health care advocacy group. Public Citizen wants the Health Care
Financing Administration (HCFA) to scrap its current method of ensuring that
hospitals meet standards for participating in Medicare. That system relies on a private, nonprofit
group to inspect 80% of the nation's hospitals to see whether they meet safety
standards required by Medicare. The other 20% are inspected by states. Critics
say the private group, the Joint Commission on the Accreditation of Healthcare
Organizations, is too close to the hospital industry and wants a public agency
to take over. The commission earns 71%
of its annual revenue from the organizations it inspects, including hospitals,
home health agencies and labs. Only 1% of the hospitals reviewed fail to pass,
although 85% are told to make improvements, according to the commission. The commission said it welcomed the report
and pointed out areas in which the inspector general praised its work. It said
it is already making changes
including a consumer complaint hot line.
The report also chastises HCFA for not having enough oversight of the
inspection program. In a statement, HCFA administrator Nancy-Ann DeParle said
the agency would adopt many of the recommendations. Those include calling for
more unannounced inspections and setting additional performance standards.
***************************************************************************
Fort Lewis, Washington, Posted 2:24 p.m.
March 16, 1999. Retired Army Major General David Hale is pleading guilty to some
of the charges against him. His attorney announced today that Hale has cut a
deal with military prosecutors in Washington State. Hale was accused of having
sexual relationships with some of his subordinates' wives.
Copyright 1999 by The Associated Press
***************************************************************************
1998 IN A NUTSHELL
By The Associated Press
A MONTH-BY-MONTH LOOK AT NOTABLE NEWS IN
1998:
June 20 - Civilian lawyer Kelly Theriot
accepts $500,000 settlement for claims an Army colonel sexually harassed her
Mistrial
Declared in Army Sexual
Harassment Retaliation Case
Army civilian lawyer Kelly Theriot claimed
that Col. Darrel Porr sexually harassed her and then conspired with other top
officers to retaliate against her when she complained. Her case was declared a
mistrial Saturday. The judge in the
case declared the mistrial after jurors said that they could not reach
agreement after four days of deliberations. Theriot said that she would pursue
a new trial. "I'm not going to quit. Absolutely not," she said.
Darrel Porr, who was deputy commander of Madigan Army Medical Center at the
time of the alleged harassment, has denied all wrongdoing.
Feminist News Stories on Sexual
Harassment, Assault and Discrimination in the Military [Source: AP - May 23, 1998]
***************************************************************************
11 May 1998
Editor
Tacoma, Washington
Dear Editor:
I am an U.S. Army physician now stationed
at Madigan Army Medical Center, Tacoma, Washington. I graduated medical school
and completed two residencies as part of my Army Medical Corps training. I am
board certified in both emergency medicine and internal medicine. I will
complete 15 years of service as an Army doctor later this year.
During my previous assignment, I was Chief
of Emergency Medicine at Landstuhl Army Regional Medical Center (LARMC) in
Germany from 1993 to 1996. As a result of the draw down of U.S. forces in
Europe, Landstuhl became the only U.S. military medical center in Central
Europe. In my capacity as Chief of Emergency Medicine at LARMC, I sought to
insure that we had the resources necessary to render the high standard of
medical care expected.
Beginning in approximately mid-1994,
however, the former LARMC Deputy Commander for Clinical Services (DCCS),
Colonel (COL) David Lipsi, and the former Chief of Ambulatory Care, Lieutenant
Colonel (LTC) David Gillingham, began to issue some orders that I knew would
endanger the lives of certain emergency patients. Both doctors referred to COL
(Promotable (P)) Kevin Kiley, the Commander of LARMC at that time, as the
source of those orders. In this setting, they gave me orders that would have
required me to abandon care of a number of civilian patients who were unstable,
and to utilize ambulances with inadequate brakes and inadequate airway
management equipment as Advanced Life Support Vehicles. Furthermore, they both
ordered me not to report deficiencies in writing. As Chief of Emergency
Medicine, I refused to carry out these orders because our patients' welfare
would be endangered. Moreover, I documented problems in the Quality Assurance
minutes of my department; LTC Gillingham suppressed distribution of these
official documents, saying that COL (P) Kiley had ordered him to do so.
Emergency care personnel at LARMC became
subject to actions that we considered to be reprisals, including understaffing
in the emergency room and orders for certain personnel to work in violation of
medically ordered restrictions (medical profiles). Both COL Lipsi and LTC
Gillingham indicated that these orders had come from COL (P) Kiley, now
Brigadier General (BG) Kiley.
In June
1995, while I was Chief of Emergency medicine at LARMC, a tragic case of brain
injury occurred in a now mentally impaired teenager currently living in
Hilton Head, South Carolina. During his initial visit to LARMC on a Saturday,
shortly after sustaining an extended loss of consciousness, he was seen by LTC Gillingham,
the Chief of Ambulatory Care, who sent him home with a listed diagnosis of
abrasions.
I was called on the child's second visit
to the LARMC emergency room the next day, Sunday, and was able to save his life
by trauma resuscitation and stabilization and immediate transfer to nearby
Kaiserslautern Neurosurgical Center for immediate surgery. I followed the
emergency trauma standard of care, based on "worst case scenario."
Our standard practice at LARMC Emergency Room had always been to assure the
highest level of specialty care available in the vicinity. The usual practice
for high-risk neurosurgical patients at LARMC ER during the weekend was to
transfer them by Advanced Life Support ambulance to either Homburg or
Kaiserslautern where an immediate operation could be performed.
Because the tragic situation clearly
revealed that such "worst case scenario" thinking had not been
utilized by LTC Gillingham on the youth's first visit to the ER, both COL Lipsi
and LTC Gillingham focused criticism on my lifesaving stabilization and speedy
transfer of the boy on the second day. COL Lipsi asserted, without my receiving
due process or peer review, that the brain damage which ultimately resulted was
because I transferred the boy to immediate neurosurgical care without waiting
the (inordinate) time required to wait for our one neurosurgeon, who was
"on call" 24 hours daily for all of Central Europe and the
surrounding vicinity (an unreasonable responsibility to require of any
specialist), and a surgical team to be called in.
Both COL Lipsi and LTC Gillingham
intensified reprisals against other emergency personnel, and me in order to
minimize any adverse exposure of LTC Gillingham's care of the boy. On Monday
June 12, 1995, COL Lipsi ordered me to his office and issued me an angry
reprimand regarding my decision to transfer the moribund child to the nearest
brain injury surgical center. He wrote out an order for me to convey to the ER
nursing staff which directed them to call in our LARMC consultants via telephone
and beeper, which was of course already our method of calling in specialists.
At the end of the one hour reprimand
session, COL Lipsi issued me the following threat, which I quote verbatim:
"LTC Smith, we do not shoot Army physicians who are uncooperative;
however, there are other things that we can do. You do not want to end up like
Dr. T, do you?" (referring by name to the OB-GYN chief whom the previous
year COL Lipsi forced to work at a high risk labor and delivery unit with
inadequate physician staffing. Dr. T suffered a situational major depression as
a result of COL Lipsi's deliberate understaffing; COL Lipsi then issued
reprisal orders for Dr. T to work in violation of his medically ordered work
restriction (medical profile).)
LTC Gillingham continued to order me to
force a seriously depressed young captain to work as a full-time emergency
physician, even though that captain's military psychiatrist had issued strict
orders (which I reported in detail to both COL Lipsi and LTC Gillingham) for him
not to work in the LARMC ER. I refused LTC Gillingham's dangerous order
multiple times, and insisted on an immediate replacement for the young captain.
In July 1995, the senior RN's and senior
medics of LARMC's ER told LTC Gillingham that they would stage an immediate
work stoppage if LTC Gillingham did not immediately agree to replace the young
impaired physician, and if he did not cease his reckless endangerment of ER
patients. I informed COL Carolyn Bulliner, LARMC Chief Nurse, and COL Jewett,
Chief of Psychiatry, of the reckless endangerment of LARMC emergency patients
by LTC Gillingham and COL Lipsi. COL Bulliner had already become alarmed at the
risk that the deliberate understaffing of Emergency Services was causing toward
patients and staff. She wisely kept the best trauma and resuscitation nursing
staff in the critical care areas, although they were due for rotation to other
services. Earlier in the summer, she had ordered Major Michael Kusek,
psychiatric RN, to institute a suicide watch to protect LARMC Emergency Room
staff from major depression induced by the reprisals of LTC Gillingham and COL
Lipsi. Psychiatry Chief COL Jewett said in the presence of witnesses he would
intervene with COL (P) Kiley, and directed me at the same time to write a Memorandum
for Record through COL Lipsi to COL (P) Kiley requesting immediate written
guidance from COL (P) Kiley about how
to proceed.
COL Lipsi then called me to his office,
reprimanded me, and refused to forward my Memorandum to COL (P) Kiley. LTC Gillingham issued angry reprimands to
myself and other ER staff, then asked COL (P) Kiley to reprimand me, when I
complained in the presence of the LARMC ER Quality Assurance RN and LTC
Gillingham that he (LTC Gillingham) was intentionally staffing the ER in a way
that was dangerous to patients. In fact, COL (P) Kiley himself reprimanded me
for my refusal to follow LTC Gillingham's orders which would have endangered
patients; I informed COL (P) Kiley that such understaffing ignored guidelines
for safe staffing published by the Office of the Army Surgeon General's (OTSG)
Consultant for Emergency Medicine. In addition, COL Kiley allowed a work
schedule to be imposed on emergency personnel that violated certain medical
profiles (work restrictions), thereby endangering both patients and staff.
In February 1996, I reported these and
other problems to the LARMC Inspector General (IG) and then informed COL (P)
Kiley that I had done so. Approximately 2 hours after I informed COL (P) Kiley
of my IG complaint, COL Ney Gore, cousin of Vice-President Al Gore, indicated
that COL (P) Kiley had ordered him to suspend my credentials to practice
medicine. COL (P) Kiley ordered me to be sent to Madigan for psychiatric
evaluation. My psychiatrists, who were treating me for depression, told me
that, when they asked COL Kiley whether I would receive due process to protect
my career and my medical credentials, he said something to the effect of,
"Just get him out of here as fast as possible!"
At Madigan, an Army psychiatrist, Major
(MAJ) Scott McDonald, assigned as my physician, obeyed telephone orders from
COL (P) Kiley to keep me hospitalized for 3 weeks on a locked ward and at Level
I (the highest) restriction, when neither the intensity nor the length of
restriction was medically indicated.
At that time, the Deputy Commander for
Clinical Services supervising all Madigan physicians was COL (P) Darrel Porr,
now Brigadier General Porr. Then COL Porr was presumably aware that a senior
Army doctor from Germany had suddenly been ordered confined to a psychiatric
ward in his hospital. COL Porr, however, later left Madigan and has yet to
explain what role, if any, he played in the abrupt psychiatric imprisonment of
an Army doctor shortly after he reported real problems with the quality of
patient care to an Army Inspector General.
I was eventually released from the
psychiatric ward and allowed to stay at Madigan and practice medicine again,
but concern about retaliation for continuing to insist that all these matters
be thoroughly and honestly investigated has not gone away. In October1996, I
submitted a formal complaint to the Department of the Army Inspector General
(IG) about the endangerment of emergency patients at Landstuhl by senior Army
medical officers. I also informed certain Senators and Representatives and
requested congressional action to prevent recurrence of such matters. I
reported endangerment of LARMC emergency patients and staff by COL Lipsi and
LTC Gillingham who said they were responding to orders from COL (P) Kiley.
Approximately one year previously, a LARMC
OB-GYN physician had made a similar complaint against COL Lipsi. That complaint
charged COL Lipsi with issuing orders to reduce staffing below safe limits in a
high-risk labor and delivery unit. Moreover, there is documentation of COL
Lipsi's reprisal orders to the same OB-GYN physician to work in violation of
his medically ordered work restriction (medical profile). Furthermore, COL
Lipsi had reportedly enforced dangerously low staffing on the labor and
delivery unit as reprisal against its Chief. These events happened while COL
(P) Kiley, an Obstetrician-Gynecologist like the OB-GYN Department Chief, was
Commander of LARMC and COL Lipsi's boss.
In September 1997, LTG Ronald Blanck,
Surgeon General of the Army, invited me to the Army Medical Command (MEDCOM) in
San Antonio, TX to provide information about my allegations. This trip was
arranged as official paid travel (TDY) orders. At LTG Blanck's request, I briefed
Quality Management (QM) personnel at MEDCOM about these matters. Those present included 2 QM physicians, one
Registered Nurse (RN), and an Army lawyer representing MEDCOM. I subsequently
met with a representative from the Army's Criminal Investigation Division (CID)
and provided related information and documentation. In the several months since
I went to MEDCOM, I have received no report from LTG Blanck's office about what
action is being taken to address the problems I exposed. I have recently learned
that BG Kiley, the former LARMC Commander, is now assigned to LTG Blanck's
office in a leadership position. If the Army Surgeon General's Office is going
to investigate, the investigation will have to include past actions of a
General Officer now assigned to that Office.
The Department of the Army Inspector
General and MEDCOM have yet to produce a Report of Investigation (ROI) about
these matters. Furthermore, last year I
was informed that the Department of the Army Inspector General assigned in
overall supervision of my case was Major General (MG) David Hale. I have
recently learned that MG Hale precipitously left active duty under a cloud
earlier this year.
Several months after my abrupt departure
from LARMC in 1996, another LARMC case, the "death of Baby V
case," was reported as a complaint to the offices of LTG Blanck and
Congressman Henry Hyde. The complaint and related information, which I have
seen, describe a situation at LARMC in which Baby V's father, who was a
military doctor, did not want to have a child with a birth defect and sought
LARMC permission to allow his yet unborn child to die without treatment.
According to the complaint, the baby's father gave a LARMC ethics committee
misleading prenatal information and, when the ethics committee was unable to
reach a unanimous decision, COL (P) Kiley reportedly made a command decision,
before the child was even born, to allow the father, a military doctor, to
withhold treatment once the child was born.
When born, Baby V had a condition
(meningomyelocele) that is easily repairable by remedial surgery, but often
fatal if not repaired. The baby was allowed to leave the hospital without
corrective surgery and died of meningitis within 2 weeks. Two families had
reportedly offered to adopt the infant in order to save her life, but this
offer was reportedly refused. COL (P) Kiley's decision, made before Baby V's
birth, created a situation that apparently permitted Baby V's death. The
circumstances surrounding Baby V's birth and death need to be investigated.
The three cases (Dr. T, the February 1996
LARMC Inspector General case, and Baby V) show repeated endangerment of patient
welfare under one Army Medical Center Commander, who should be required to
account for his own role in the events described. Both of my Army Medical Corps
Residencies-Emergency Medicine at Madigan Army Medical Center (where I have
returned) and Internal Medicine at Eisenhower Army Medical Center-have taught
me to uphold the standard of care for the patient's welfare. Neither of these
centers would tolerate retaliatory actions against physicians and nurses that
endangered patient care.
I notified my chain of command last year
that the request for investigation had gone to LTG Blanck, and that it would
become public knowledge eventually. On Monday, 4 May 1998, I notified my
superior officer, the Chief of Emergency Medicine at Madigan, that I would soon
be contacting the press about these matters.
Before other patients are harmed, I
request an immediate congressional investigation regarding the now
long-reported orders of BG Kiley, COL Lipsi, and LTC Gillingham at LARMC. In
accordance with Section 846 (Safeguarding of military whistleblowers) of Public
Law No. 100-456, otherwise known as the Boxer-McDermott Whistleblower Protection
Law, I continue to request career protection from appropriate Members of
Congress in keeping with the law's intent to protect military whistleblowers
from retaliation.
Over two years have passed since I
originally reported these problems and was confined to a psychiatric ward after
doing so. The quality and integrity of the Army medical system are vital to the
taxpayers who support it, to the parents who entrust their sons and daughters
to it, and to the men and women in uniform who must rely on it. Congress must
act if the Army is unwilling or unable to do so.
Thank you for your attention.
Respectfully,
Stephen Whitlock Smith, MD
Fellow,
American College of Emergency Physicians
Fellow, American College of
Physicians
Lieutenant Colonel, US Army Medical
Corps
Steilacoom, WA 98388
Cc:
Lieutenant General Ronald Blanck, Army Surgeon General
Brigadier
General George Brown, MAMC Commander
Madigan
Army Medical Center Public Affairs Office
Representatives
Dicks, McDermott, Pelosi, Spence
Senators
Boxer, Feinstein, Thurmond
For
Record
***************************************************************************
Friday 9
October 1998 0830 CID Agent Navarro, Fort Lewis, Washington 98433
Spell corrected copy submitted Friday 23
Oct 1998 1230
I, Stephen Whitlock Smith MD (LTC, USA MC)
024-38-5114, report what I believe to be criminal wrongdoing by high-ranking US
Army Medical Corps Officers and others at Madigan Army Medical Center and other
locations. I believe that the intent is a cover-up to protect Brigadier General
Kevin Kiley and others from charges of reckless endangerment of emergency
patients and medical staff at Landstuhl Army Medical Center.
I met Dr. Sue Bailey, Assistant Secretary
of Defense for Health Affairs, at 1130 hours on 1 September 1998, on the
occasion of the inauguration of TriCare Senior Prime (Medicare) Subvention by
Madigan, directly in front of the Reception Desk of the Adult Primary Care
Clinic where I am assigned as Acute Care Physician for TriCare Senior Prime.
Sue Bailey is a classmate at George Washington University Medical School,
Washington, DC, and we reminisced about our medical school.
Three minutes after our short meeting, I
was approached by a very angry officer whom I had never met, who left the
Madigan Command Group at high speed after exchanging words with COL Casey
Jones, Madigan Deputy Commander, and others of the Command Group. This officer
demanded to know my place of duty, and I replied that my duty station was
immediately in front of us at the Adult Primary Care Clinic where I am Acute
Care Physician for TriCare Senior Prime patients. The angry officer still did not formally identify himself. I
noticed his name plate "Hill" and grade of Brigadier General, and
asked him if he was to be our new Madigan Commander. He did not directly reply.
I said good-bye and told him that I would be rejoining Dr. Sue Bailey at 1300
for her scheduled tour of our clinic. The officer then rejoined the Madigan
Command Group and exchanged words with COL Casey Jones, Deputy Commander, and
others.
At 1305 hours on 1 September 1998 I was
waiting outside the Commander's Conference Room in the vicinity of Mr. Mike
Meines and Ms Sharon Ayala of Madigan Public Affairs, in discussion with LTC
Steve Carter, Madigan Troop Commander. LTC Carter called my attention to
someone waiting to speak to me directly behind me, and I turned to see who it
was.
I recognized Mr. Cleaver, Brigadier
General Brown's security agent. Mr. Cleaver called me by name. "LTC Smith,
I need to speak with you." He began
to ask me a question, then stopped in mid-sentence when he noticed that my name
badge was missing.
Mr. Cleaver then spoke to me angrily,
"Do you know that you are not wearing a name badge?" I replied that,
because I was wearing my Class A uniform for the occasion, I must have
forgotten to transfer my name badge from my duty uniform. I asked Mr. Cleaver
if he would issue me a replacement badge. He then escorted me hastily up one
floor to the Provost Marshal's Office with one arm behind me pulling me. We
entered his office; he ordered me to
remain seated. Mr. Cleaver sat at his desk facing me, and said, "What are
your intentions regarding Dr. Sue Bailey?" I replied that Dr. Bailey and I
had attended George Washington University School of Medicine in Washington, DC.
Mr. Cleaver said that the Commander, or
the Command, (I did not hear clearly
which word he used) accused me of carrying a concealed weapon. He said, "I
might have to pad you down for concealed weapons!"
I replied that he could certainly search
me. I said that I was being accused falsely. I said, "I am a physician
known to you and to the Command. I believe that I will need to report this
incident."
Mr. Cleaver asked me sternly, "Why
are you helping to lead the tour for Dr. Sue Bailey? You are not a chief; you are ordered to return to your duty
station and stay there. You are directed to ask your chief to lead the
tour."
Mr. Cleaver then allowed me to leave his
office, and with an arm pushing me from behind my back and right hip, forced me
to walk down the escalator toward the Information Desk of the Medical Mall. At
that point, I tried to stop on the first floor and request clarification of Mr.
Cleaver's orders. He then pushed me down the escalator leading to the Adult
Primary Care Clinic, ordering me to stay on that level.
I returned to my Clinic, and asked my
Clinic Chief MAJ Richard Jordan to lead the tour in my place, telling him and
Clinic Administrator MAJ Rumph that I had been ordered by the Command to do so.
All three of us waited one hour, and then Ms Sharon Ayala notified us that the
tour through our clinic had been canceled.
I sought legal counsel and reported these
happenings via memoranda to Dr. Sue Bailey, as well as to Secretary of the Army
Caldera and Secretary of Defense William Cohen. I requested an investigation in
the nature of an Article 138 investigation.
On 1 October 1998, I received an urgent
e-mail message from LTG Ron Blanck's MEDCOM Quality Management Office in San
Antonio, Texas, that an investigation which I and others had requested into
reckless endangerment of emergency patients and staff at Landstuhl Army Medical
Center, was suddenly being moved to Germany. (I observe here that the
principals of the investigation, including Brigadier General Kevin Kiley, COL Ney
Gore, COL David Lipsi, and LTC David Gillingham, are no longer in Germany; in
fact, BG Kiley is in San Antonio, Texas, and COL Gore is in El Paso, Texas. Nor
are any of the principal 65 witnesses to the investigation any longer in
Germany. Nor are any of the medical records of the reckless endangerment cases
available in Germany, since many Medical Treatment Facilities there keep
emergency records for only one year after the day of treatment. It has been
over 2 years since I initiated my request for investigation.)
On 1 October 1998 at 1400 hours, my Clinic
Chief MAJ Richard Jordan informed me that COL Casey Jones, Madigan Deputy
Commander, had given him an angry direct order for me to submit all of my
medical records for review by close of business that day.
On 5 October 1998, I was called by Ms
Lissette Ortiz into the office of MAJ Richard Jordan. MAJ Jordan did not start
the meeting until 2 minutes later when MAJ Rumph arrived as a witness to the
meeting. MAJ Rumph took detailed notes throughout.
MAJ Jordan handed me a counseling
statement signed by himself which informed me that my credentials file was at
risk of being subjected to adverse action. I then reported the detention by
Brigadier General Brown's security agent of 1 September 1998 as reprisal for my
having spoken to Dr. Sue Bailey, Assistant Secretary of Defense for Health
Affairs.
At 1300 hours on 5 October 1998, I
reported the foregoing events to my Department Chief COL Lester Reed, and to my
former Department Chief COL Matthew Rice.
At 0800 on 8 October 1998, MAJ Richard
Jordan informed me that there were "no issues," and that I could send
him 2 charts per day for his review, instead of the previous 100%.
I believe that recent events as described
above relate to my report to Brigadier General Kevin Kiley on 12 February 1996
in the presence of Ms Michelle Jung, of reckless endangerment of emergency
patients and staff, and the intentional orders for medical personnel to work in
excess of medical work restrictions ("profiles," ordered by Landstuhl
physicians, to protect personnel from serious illness.)
I reported in detail Brigadier General
Kiley's prompt orders to suspend my credentials, and to transfer me out of his command, with no recourse to the
due process required by Regulation and
Statute. The specific steps which are in violation of established Regulations
and standards have been reported in detail by myself and by COL Robert
Tabachnikoff. I referred LTG Blanck's Quality Management Division to my
attorney, Mr Mike Gaffney, and to Dr.
Tabachnikoff's attorney, Mr Barry Steinberg, both of Washington, DC. To my knowledge, neither LTG Blanck's Office
nor LTC Ed Bodling of the Department of the Army Inspector General ever
contacted either attorney's office for a complete listing of violations and
unlawful orders.
At the time of my suspension from medical
duties as Emergency Medicine Chief on 12 February 1996, I was also the Medical
Staff Joint Commission Representative, and I was reporting directly to LTC
Debra Spittler and to COL Ney Gore, Deputy Commander.
BG Kiley's orders to remove me from his
Command, and his orders to COL Gore to order removal of extra copies of my
Inspector General Complaint, served to accomplish the following:
To prevent my report of significant
deviations from Joint Commission Guidelines, to include the following.
1.(JCAHO Standards 1996)
RI.1.1 The patient's right to treatment or
service is respected and supported.
RI.1.3.1 Confidentiality
RI.4 The hospital operates according to a
code of ethical behavior
PF.1.7 Patients are informed about access
to additional resources in the community.
CC.1 Patients have access to the
appropriate type of care
CC.8 An established procedure is used to
resolve denial-of-care conflicts over care, services, or payment
LD.2.4Directors recommend a sufficient
number of qualified & competent persons to provide care
HR.2The hospital provides an adequate
number of staff members whose qualifications are consistent with job
responsibilities
MS.1.1.3 All medical staff member and all
other with delineated clinical privileges are subject to medical staff and
departmental bylaws, rules, and regulations, and policies and are subject to
review as part of the organization's performance-improvement activities.
MS.3.1.6.1.7 The mechanism for fair-hearing
procedures
MS.5.2 There are mechanisms, includinq a
fair hearing and appeal process, for addressing adverse decision for existing
medical staff members and other individuals holding clinical privileges for
renewal revocation, or revision of clinical privileges .
MS.8.1.6 Significant departures from
established patterns of clinical practice.
MS.2.3.4.1.3 The conditions and mechanisms
for removing officers from their positions:
MS.3.1.6.1.6 The mechanism by which
medical staff membership may be terminated:
MS.3.1.6.1.7 The mechanism for
fair-hearing procedures.
TX.M.6.1.1 Seclusion or restraint is use
only to prevent the individual from injuring himself or herself or others, or
to prevent serious disruption of the therapeutic environment.
MS.2.3.2 Fair-hearing and appellate review
mechanisms for medical staff members and other individuals holding clinical
privileges:
2. In addition, I had knowledge of serious
deviations from Nuclear Regulatory Standards for shielding and removal of used
radioisotopes at Landstuhl.
3. Deviation from standards to include
Department of Transportation, DOD, German, regarding operation of Advanced Life
Support Ambulances.
4. Evidence of Black Market activities
involving US Government Ambulances in the Landstuhl-Kaiserslautern area: as
reported by Landstuhl Paramedic SSG Robert Barrett to "Waste Fraud and
Abuse Hotline" via protected communication; by SSG Charles Marmann and SGT
Mark Major and MAJ Laurie Sandstrom via our Departmental Minutes and directly
through the Nursing Chain of Command. Agent Zangerine of Fort Sam Houston CID
confirmed to me in September 1997 that such a Black Market was present. I
believe that the existence of such black market operations prevented BG Kiley
from granting our requests for acceptable Advance Cardiac Life Support
Ambulances.
5. Evidence of Continued Credentials Libel
by COL David Lipsi, as well as his direct orders to me to falsify a credentials
document in favor of LTC David Gillingham. (Sources at Medical Claims, Madigan,
where Gillingham had been assigned immediately before Landstuhl, have informed
me that Gillingham had left Madigan for Landstuhl under some form of
credentials restriction because of several unresolved medical claims against
him.) COL Lipsi had been reported previously for intimidation of witnesses in
regard to credentials files, in line with the report by DOD Inspector General
to William Cohen, as well as to other members of the Senate Armed Services
Committee.
6. Reckless endangerment and cover-up of
marked deviation from standards of care in numerous cases of emergency
conditions at Landstuhl. One case, as reported publicly in the Hilton Head
Island Packet, July 1998, involved a denied claim for $7.5 million in a case of
brain injury in a child. Some witnesses for some cases have told me that they
have already suffered reprisal.
7. I have already reported evidence of the
involvement of high-ranking officers at Madigan in reprisal against myself and others,
seemingly to prevent investigation of the charges against Brigadier General
Kevin Kiley and those who said that they were following BG Kiley's orders.
8. My report to LTG Blanck and to the
McClatchy News Service of 11 May 1998 occurred during the same time period as
the $500,000 settlement from Department of the Army, to Ms Kelly Theriot,
former JAG Chief of Madigan, who had reported alleged wrongdoing by high
ranking officers at Madigan. Previous to my 11 May report (released through the
Madigan Chain of Command) COL Casey Jones, Deputy Commander, had informed my
chief COL Matthew Rice that LTC Smith will NEVER receive full credentialing at
Madigan. However, on 13 May 1998, the Credentials Committee under Chairmanship
of COL Jones granted me Internal Medicine Credentials, and left my Emergency
Medicine Credentials intact.
Other documentation will be sent as
required.
I request career protection under PL
100-456 and all applicable regulations and statutes per Members of Congress. I
believe that a cover-up of immense proportions is underway to protect
high-ranking officers from charges of wrongdoing. The accusations which I and
others have made involve specific reckless endangerment of US Army emergency
patients, and reprisals against those reporting such problems.
Stephen Whitlock Smith, MD
Graduate, George Washington University
School of Medicine US ARMY Health Professions Scholarship Program
Graduate, US Army Internal Medicine
Residency, DDEAMC, 1983
Graduate, US Army Emergency Medicine
Residency, MAMC, 1987
Acute Care Physician, TriCare Senior Prime
(Medicare) Adult Primary Care Clinic, MAMC
cc:
Senators Thurmond, Feinstein, Boxer
Representatives Dicks, McDermott, Pelosi
General Accounting Office
Joint Commission (JCAHO)
Memorandum for Record
***************************************************************************
UNDER FREEDOM OF INFORMATION AND PRIVACY
ACTS
Brigadier General Mack Hill
Commander
Madigan Army Medical Center
Tacoma, WA 98431
2 January 1999
Dear General Hill,
Pursuant to provisions of Article 138 of
the Uniform Code of Military Justice I am requesting of you the following:
O Cessation of any adverse career actions
against me; and
O Your consideration of providing
documents to me as detailed below; and
O Your facilitation of my request, sent
last week via personal correspondence to COL Casey Jones, Chairman,
Credentials, for specifics related to a Credentials Hearing.
I request the copies of the following
documents or files pertaining to me which are either maintained at MAMC or
reside in files at MAMC:
O A complete copy of my individual
Clinical Credentials File
O Any DOD, DOD (HA), HQDA, Army, AMEDD,
MEDCOM, MAMC correspondence, documentation, notes, letters, email record or
other records, or other documents (hard copy or electronic) received,
maintained, retained or on file in the Credentials Office or in the files of
Credentials Committee, or in the personal file of its Chairperson or in the
personal file of the DCCS or Commander regarding my credentialing and
privileging since February 1996 which are not already included in my individual
Clinical Credentials File
O A complete copy of my individual
Provider Activity File
O A complete copy of my individual Madigan
Health Provider Program file
O Minutes of any and all Credential
Committee meetings, regular, special and or ad hoc in which actions or
discussions regarding me, my credentials and privileges appear
O Minutes of all Hospital/Center Morning
Reports, Teaching Chiefs, Center and or other command meetings, conferences or
briefings which reference me or in which there are actions or discussions
regarding me, beginning from February 1996
O Copies of each published and approved
the MAMC Officer Evaluation Reports rating scheme from Feb 1996 through today
O Official copies of the Order detaching
me or reassigning me from permanent party status at LARMC to patient status
with MHC LARMC
O Official copies of the Order placing me
in medical evacuation status from LARMC to CONUS with ASMRO bed designation
details
O Official copies of the Order attaching
me or assigning me to patient status with MHC MAMC
O Official copies of the Order detaching
me or reassigning me from patient status with MHC MAMC to permanent party at
MAMC
O Official extracts of morning reports (DA
Form 1) and Command Interest summaries reflecting my status as depicted in the
orders above
O E-mail messages received by MAMC Public
Affairs or any official in the Command Group referencing me and my protected
communications associated with any and all detailed Inspectors General or DOD
officials, AR 15-6 Investigating Officers, CID Agents or any other body
conducting or having interest in Official Investigations in which I am named as
a subject, suspect or witness
O Records, memoranda, and written
summaries of any conversations between yourself and other Department of Defense
or Government Employee, Public Affairs Officers or any official referencing me
and my protected communications associated with any and all detailed Inspectors
General or DOD officials, AR 15-6 Investigating Officers, CID Agents or any
other body conducting or having interest in Official Investigations in which I
am named as a subject, suspect or witness
O A copy of the most recent JCAHO report
for MAMC, to include observations and findings regarding medical records. What
is requested is the detailed report with deficiencies issued by the Commission
by mail a few weeks after the survey, not the score matrix issued on the last
day of the visit.
O the DAC job description of the Physical
Security Agent, Mr. James Cleaver, that was current as of 1 Sep 98.
O Extracts of the DAC Civilian Personnel
file for Mr. James Cleaver, demonstrating the training he received in
preparation for his current job position as Physical Security Agent.
O Copies of any records and or files
bearing my name appearing in or referenced in Congressional Correspondence
regarding alleged reckless endangerment of emergency patients at Landstuhl
and/or any alleged cover-up thereto.
Sincerely,
Stephen Whitlock Smith, MD
Cc: Legal Counsel
NOTHING FOLLOWS
***************************************************************************
APPEAL TO DR O’LEARY AND MR MANCUSO 18
October 1999
Dr O’Leary and Mr Mancuso,
The following is my Appeal:
Corresponding to specific documents to be forwarded----------------
The following questions relate to each
credentials document mentioned:
#Notification of restoration of clinical
privileges by DCCS COL Pat Kelly 2 april 99.
Why was there such a prolonged delay until
COL Gilman partially restored my clinical privileges 4 days after the Army
Times article in July? Since the psychometric test which imposed supervision on
my credentials originally is still missing, should not the provision for
supervision be waived?
Credentials Hearing Minutes 10 February
1999
#2 (page)
What is your opinion of the effect of the
rapid turnover of JAG officers (Army attorneys) in this credentialling action?
Are all legal questions the province of
LTC Pearson, LTG Crocker's JAG who presided over much of the hearing
proceedings? Alternately, is COL Woodling, LTG Crocker's Chief JAG Officer, the
responsible legal authority?
Why did BG Hill not provide me a Trial
Defense Lawyer in conjunction with his memorandum to me of 2 February 1999
delivered in person by CPT Geib. Could your office provide me with a Trial
Defense Attorney in case BG Hill is still unable to do so? How am I to
determine if I require a Trial Defense Attorney, if LTG Crocker's JAG officers
all seem to have divergent opinions on this matter?
#3
If the Impaired Provider Committee reports
by MAJ Jordan (August, September, and October 1998) were considered in these 10
February minutes, why did I not receive my own copy of these until 1200 noon on
3 March from Ms Carole Meines. These evaluations written by MAJ Jordan, my
supervisor, were important in the Credentials Committee actions during the
months of August, September, October, and November, 1998. What was BG Hill's
reason for withholding this feedback from me during my patient care time in the
Department of Medicine? Did BG Hill make such a decision before or after the
conversation which he had with me on 1 September 1998 immediately after Dr Bailey
and I chatted. What was the reason for allowing me to see my supervisor's
evaluations of August-October 1998, for the first time on 3 March 1999, and
only in response to my request to BG Hill under the Freedon of Information Act?
#4
Each of the JAG officers associated with
this hearing offers a different opinion regarding the question of whether
witnesses can see credentials documents about which they are asked to testify.
All of my witnesses asked me for specific written guidance in order to prepare
them for the hearing. The discrepant opinions of CPT Geib, LTC Pearson, COL
Woodling, and MAJ Cusker on this point were impossible to resolve to my
witnesses' satisfaction. Consequently, only 2 witnesses were willing to testify
on behalf without any written guidance. Moreover, Dr.Bailey testified by letter
without hesitation. When will I be allowed to bring forward the other
witnesses' testimony? Dr O’Leary and
Mr Mancuso, what is your opinion in
this regard?
MAJ Cusker is my JAG officer assigned by LTG
Crocker for the still-pending complaint against BG Hill for his role in my
detention by Mr. Cleaver on 1 September 1998 after my conversation with Dr. Sue
Bailey. Why then, did LTC Pearson prohibit MAJ Cusker from advising me
regarding witness preparation for the Credentials hearing? Dr O’Leary and Mr
Mancuso, I would like your opinion of
this point because the witnesses for both proceedings are the same witnesses,
and the evidenciary documents in question are the same documents.
#5
I reported that there was erroneous
information in the credentials records relating to me. I asked several times that these errors be
corrected at time of the hearing. LTC Pearson's judgment was that these errors
should not be corrected during the hearing itself. Since the information
relates to my own medical record on file at MAMC which does not support the
erroneous information in the minutes, when will such errors be corrected?
One obvious error describes my medical
condition as "catatonic." Another error is the wording "manic
depressive." Both my official MAMC records and Dr. Dunner's report from 10
May 1999 fail to support these diagnoses. When will these errors be corrected
within the credentials records?
The following crucial MAMC medical files
relating to me were reported missing between 1 and 10 May, the day of the
Independent Medical Examination at University of Washington: 1) MAMC Outpatient
Psychiatry Record; 2) MAMC Outpatient Psychology Record; 3) Psychometric Test
and Report. These records are critical in supporting my witnesses' account of
events. COL Victor Bell, former Chief of Psychiatry at MAMC, was the member of
the Credentials Committee who discussed BG Hill's referral of me to Dr Dunner
of UW, and arranged the transfer of medical information to Dr. Dunner. However,
BG Hill has now reassigned COL Bell to Alaska. How can the information in the
missing files be obtained or reconstructed?
In particular, Dr O’Leary and Mr
Mancuso, COL Gilmore arrived as new
Deputy Commander at approximately the same time the records were discovered
missing. Could you please investigate what his role is or will be in finding
the missing records?
#6
MAJ Cusker is the JAG officer assigned to
me by LTG Crocker in order for me to defend against BG Hill's personal
involvement the events of 1 September 1998. MAJ Cusker and I had extensive
discussions regarding our case during December and January. I transferred large
numbers of files and e-mail to her in order to help her to develop our case.
Why did BG Hill requisition MAJ Cusker to be the MAMC Center Judge Advocate
just as our case was being developed in January? Dr O’Leary and Mr Mancuso,
this question was presented to LTC Pearson and COL Woodling as a
question of conflict of interest. What is your opinion on this matter, and how
can it be resolved, so that the allegations which I have made regarding the
events of 1 September 1998 can be directed into the proper channel?
LTC Pearson said that the Article 138 charges
against BG Hill and the credentials hearing are 2 separate matters. Since this
involves the same exact witnesses and the same exact allegations, why are they
being treated separately? Do you intend to rule on the events of 1 September
1998, or should the matter ultimately stay within its original venue, Secretary
of the Army Caldera with the assistance of Dr. Sue Bailey?
The Army Times article of 15 February 1999
referring to the events of 1 September 1998 at MAMC was constrained by the fact
that MEDCOM Public Affairs seemed not to know any details of the event. Has
MEDCOM Public Affairs been informed of the events of 1 September 1998, and of
my FOIA request for MEDCOM-funded surveillance videotapes which I believe would
substantiate the testimony of my witnesses? When will the MAMC witnesses from
within the MAMC Command Group who corroborate my account of events be allowed
to testify?
Dr. Bailey kindly provided documentary
evidence in support of my witnesses. Should the case then be transferred to her
office for administrative decision in order to save the time required to
initiate another hearing within MAMC or MEDCOM only for the events of 1
September 1998?
With the exception of Dr. Bailey, my other
witnesses of the events of that day have declined to testify, because they are
currently members of the Command Group at MAMC. As such, they might find
themselves as witnesses against other members of the Command, namely BG Hill
and Mr. Cleaver. Could Dr. Bailey's office intervene informally in this matter,
since Dr. Bailey was present also?
Specifically, when will the witnesses of
the reported harassment by BG Hill and the detention by the security agent be
allowed to testify about the events of Sep 1 1999. These events are crucial to
the case.
#7
What is your opinion whether I may utilize my credentials
documents containing information about me, in the preparation of witnesses on
my behalf? Why were the Freedom of Information Act documents which we requested
in January not supplied before the credentials hearing?
#8
Specifically, the missing psychometric
test result of 25 March 1997 has not been received under FOIA. The test is the
determinant for the supervision of my medical privileges. Does not the
recently-obtained FOIA document from Dr Marc Williams (my physician who ordered
the psychometric test) dispute the Credentials Committee decision to impose
supervised credentials as opposed to unsupervised?
What is the meaning of the memorandum
received from MAJ Cusker on 10 February in which she attempts to justify her
representation of MAMC and the simultaneous Article 138 associated allegation
against BG Hill? Since COL Woodling's cover memorandum of the same date appears
to support MAJ Cusker's opinion in this regard, what is your opinion of how to
resolve the dilemma?
#9
Why does COL Woodling offer a new JAG
officer to my service because of the discrepancy, if there is no discrepancy?
However, why is a Trial Defense Attorney not provided?
Should I now resume working with MAJ
Cusker so that the Fort Lewis JAG
office has the opportunity to provide an investigative response to the events
of 1 September, particularly in regard to BG Hill's personal involvement?
Apparently, LTG Blanck’s JAG officer COL Phil Savoie has not intervened in this
regard.
If you are able to offer me MEDCOM JAG
support in this matter, may I request the assignment of CPT Jeannette Stone of
COL Savoie's office at MEDCOM? CPT Stone was present during the briefing which
LTG Blanck kindly enabled (via TDY orders for me) which I gave to MEDCOM
Quality Management team in September 1997 with respect to the reckless
endangerment allegations regarding Landstuhl, under then-COL (P) Kevin Kiley's
command.
#10
What was the intent of BG Hill's memorandum
of 2 February threatening punitive action if QA documents were used in
preparing witnesses? Why did BG Hill ask COL Bauman the Chief of Radiology to
sign the memorandum of 2 February? Dr O’Leary and Mr Mancuso, am I required to respond to such a
memorandum specifically in writing, since no Trial Defense Attorney was
provided for me to do so?
What is MAJ Cusker's role in this matter.
Could MAJ Cusker be assigned to me as my Trial Defense Attorney, if such
assignment is required at MAMC?
Was LTC Pearson requesting that a member
of the committee read me my rights?
Why did CPT Geib advise me of my right to
Trial Defense Attorney, but without official charges having been filed? I
believe that CPT Geib is assigned to BG Hill's Command directly. Why then would
COL Woodling, who is LTG Crocker's Chief JAG Officer be able to speak
officially for CPT Geib not of his own command? What is your opinion regarding
COL Woodling's memorandum?
Are my witnesses in the credentials
hearing the persons which BG Hill means are at risk of punitive action, or am I
at risk of this?
#11
Why did COL Woodling address both hearing
and the article 138 in his letter? Is there confusion over disclosure of
hearing minutes to attorneys vs members of DOD vs members of AMEDD? What are
JCAHO guidelines regarding disclosure of credentials documents to credentials
hearing witnesses during a credentials proceeding? What is your opinion about
which guidelines to follow, so that I can appoint proper witnesses for both
settings?
#12
Dr O’Leary and Mr Mancuso, would the safest way be to have the
documents released through the
Commander directly to witnesses? My witnesses were intimidated by lack
of clarity on this issue and decided not to testify. Is BG Hill the authority
who will determine if QA documents can be released to witnesses? If he does not
agree with respect to certain key documents, are you then the authority who
will decide this issue?
#13
BG Hill did not provide guidance regarding
the witness list. When will I receive official written guidance regarding
witnesses? Specifically, should witnesses worry that participating in a
credentials hearing might place them in any legal jeopardy?
#14
I presented no witnesses on 10 February
because of BG Hill's direction that punitive action was possible if I allowed
them to read credentials documents. Shall I send the proposed witness list to
you in order to authorize release of certain documents to certain witnesses for
the purpose of the hearing? Or should I keep such a list of names confidential
until you can guarantee their rights under Whistleblower Protection provisions.
#15
Why did BG Hill direct that the time frame
to be addressed by the credentials hearing be 1 July to 3 November? Should witnesses
be prepared only for that time period? Can documents be provided to them for
their hearing preparation which were created ONLY within that time frame, or
are you going to allow previously-created documents to be provided?
#16
LTC Pearson allowed me to consult with MAJ
Cusker once during the hearing for five
minutes, as a brief recess; however, why could she simply not be brought into
the hearing room when this issue is presented to JCAHO and DODIG for resolution?
What Army Regulation or JCAHO guideline covers the exclusion of a respondent's
counsel from the hearing room? What is your opinion, Dr O’Leary and Mr
Mancuso, whether there is conflict of
interest of the various JAG offficers involved in the case?
What is your opinion regarding the decision
by BG Hill not to assign me a Trial Defense Attorney to be present during the
credential hearing?
#17, 18
I contested COL Jones impartiality because COL Jones is a subject of the Article 138 for my detention and
physical assault on 1 September. Since BG Hill is personally mentioned in these
Article 138 allegations, why was BG Hill not allowed to recuse himself from
final judgment over the hearing findings?
The MAMC and Fort Lewis JAG officers
allowed the proceeding to continue under such conflicting opinions? If such a
conflict recurs at any time before BG Hill restores my credentials, is there
any provision for such controversies to be resolved before any other
proceedings begin?
What provision can you now afford me that
this apparent conflict in interest can be resolved, at least before a final
decision is made on my credentials?
#19
The allegations stated in the hearing
minutes regarding behavioral issues are linked with the events of 1 September
1998. Specifically, after my short conversation with Dr. Bailey in the
receiving line, BG Hill approached me with his anger seemingly directed toward
me; the detention and physical assault by Mr Cleaver, MAMC Security Officer
followed shortly thereafter. Is there still no official statement from BG Hill
regarding what he might have said or done in the minutes after he and I spoke,
which might relate to Mr Cleaver's treatment of me at the time of the
detention? Specifically, Mr. Cleaver indicated to me that I was accused by the
Command of threatening Dr Bailey in some manner. Where did such an allegation
originate?
Dr Bailey has specifically corroborated
for me in writing that she was aware of no threat to herself or her traveling
party on 1 September 1998. During the
outbriefing at Fort Lewis that day, what was the report furnished to LTG
Crocker regarding the detention and physical assault of that day. Did others in
the outbriefing furnish a statement for LTG Crocker that you could assist me in
obtaining for my defense?
Another reason that BG Hill's sworn
statement would be helpful is that he identified me my name "LTC
Smith," then shouted to me his demand that I identify my full name and
place of business. Since I had never made his acquaintance previously (he was
not yet officially MAMC's Commander), how had he identified me by name? The
rest of my chronology of the event is summarized in my sworn statement to CID
of 8 October 1998. This was made after a 5 week period of time elapsed with no
official explanation to me from BG Hill or MAMC Command Group about why such
events had transpired. Dr O’Leary and Mr Mancuso, would you please assist me in obtaining a sworn statement from BG
Hill? I believe that he deserves to provide his own official statement of that
day's events.
Because the detention and physical assault
and the behavioral issues related to the official written complaint to Dr.
Bailey, Assistant Secretary of Defense, are linked, LTC Pearson asked COL Jones
to recuse himself. Am I correct in assuming that BG Hill would likewise have been
asked to forgo officiation at such proceedings, if he had been present at the
hearing; however, his signature is required for me to renew my MAMC
credentials. Has Fort Lewis JAG office made a ruling yet regarding BG Hill's
signing my credentials record? What is your opinion regarding how such a
dilemna could be resolved?
LTG Crocker's JAG officer LTC Pearson
asked COL Jones to recuse himself. As COL Jones left the room precipitously,
there ensued some visible confusion about what would then be the next step.
After a declared 5 minute recess, which truthfully lasted 30 minutes, COL
Kelley reconvened the hearing for one minute in order to declare a three week
recess. Dr O’Leary and Mr Mancuso, what
was the legal basis for continuing the proceedings without requesting that BG
Hill not be similarly recused from participation in the credentials action?
#19, 20
The hearing minutes for 10 February are
signed by COL Kelley only. There is no signature by COL Jones (who presided over
almost the entire session). There is no signature by Ms Meines, Recorder, nor
did either BG Hill or LTC Pearson, LTG Crocker's JAG, provide their signatures.
Dr O’Leary and Mr Mancuso, do you believe that the portion of the
hearing on 10 February has had a review by any JAG officer, as required by AR
40-68?
Does COL Woodling's cover memorandum then
substitute for any required signature from LTC Pearson, CPT Geib, MAJ Cusker,
or LTC Olmsted?
Enclosures:
#4 January 1999 letter from COL Jones
Did BG Hill's letter of instruction as
signed by COL Jones have the benefit of legal review by LTC Pearson, MAJ
Cusker, CPT Geib, LTC Olmsted, or COL Woodling?
Were the instructions reviewed for
adherence to AR 40-68 15-6? Why were denials made regarding my request
for tape recording and verbatim transcript? Dr O’Leary and Mr Mancuso, the Freedom of Information Act denial from
MEDCOM states such a denial was made because neither form of hearing record was
requested by me beforehand. However, BG Hill's letter of instruction, signed by
COL Jones, verifies that I indeed DID make that request. Dr O’Leary and Mr
Mancuso, I do now request your
assistance in obtaining the full tape recording of all hearing proceedings;
such a recording would help me and my counsel to respond to marked
discrepancies which we have found in the record so far.
#8 February 1999 letter from SWS to COL
Jones
What was the implication of MAJ Cusker's exclusion from the hearing by
BG Hill? MAJ Cusker was at the time of the hearing simultaneously representing
me and BG Hill. How does this relate to the wording of COL Woodling's reply?
#9 February 1999 COL Woodling's letter
Is COL Woodling replying for LTG Crocker,
or only for the JAG officers under his direction. In COL Woodling's analysis of
the role and intent of CPT Geib, is COL Woodling speaking for BG Hill or only
for Fort Lewis? (in regard to whether CPT Geib was reading me my rights or
not.)
#2 February 1999 memorandum signed by COL
Bauman
At the 10 February 1999 hearing, Ms Nancy
Greenfield, RN, BG Hill's Quality Manager, clarified the meaning of the
memorandum and why it was delivered to me by a JAG officer (CPT Geib.) Since
COL Bauman deferred to Ms Greenfield for this explanation, did Ms Greenfield
actually write the memorandum, or did COL Bauman? Did either of them intend for
CPT Geib to read me my rights? Were Ms Greenfield or COL Bauman aware that by
limiting my ability to prepare witnesses, this might diminish the validity of
the proceedings? Was BG aware of this potential?
Have Joint Commission guidelines regarding
due process in credentialling matters, as well as right of appeal, been
considered fully in my case? Have JCAHO Offices of Quality Monitoring, rendered a judgment yet whether or not the
proceedings met their criteria?
Ms Greenfield, is MAMC's JCAHO expert. Was
her apparent direct involvement in preparation of the 2 February memorandum to
prevent me from transferring any of the hearing minutes to the Offices of
Quality Monitoring. Under AR 40-68, JCAHO
and other accreditation organizations are specifically allowed to see QA files
under certain circumstances?
Has MAMC asked JCAHO to review my case during the current accreditation phase?
#3 March Credentials Hearing
Attendance
Dr O’Leary and Mr Mancuso, why was a credentials clerk as well as the
Recorder Ms Meines allowed to participate? Was not one clerical person enough.
Why did BG Hill not allow correspondents of the media to attend, since
published reports had already appeared in advance of the 10 February hearing?
These correspondents would be able to verify whether due process had been
achieved. Would requests for media representation be again denied in any future
credentials proceedings? What is the correct way to apply for media representation
to occur?
#6 (page)
Dr O’Leary and Mr Mancuso, I can establish beyond reasonable doubt that
I arranged properly with MAMC Command and Dr Bailey to accompany her tour with
respect to my responsibilities as Tricare Senior Prime Acute Care Physician. I request that you hear the witnesses who
can verify this. Those specific witnesses were not afforded the opportunity to
testify for me on 3 March.
#8
Dr O’Leary and Mr Mancuso, a sworn statement from BG Hill is missing
from this hearing record. What were his actions on 1 September 1998? What
communication, official or unofficial might he have had with Mr. James Cleaver,
MAMC Security Guard?
#9
Dr O’Leary and Mr Mancuso, even a brief examination of LTC Foster's
typewritten statement will show that it is not a properly sworn statement. It
is rendered on a "sworn statement" standard form; however, it is not
accompanied by a witness signature.
Without ANY STATEMENT at all from BG Mack Hill to explain his own
actions that day, we are left only with Mr Cleaver's statements under oath. Mr
Cleaver is accused in my testimony to CID of 9 October 1998, with physically
assaulting me by shoving me down the Medical Mall escalator. It is necessary to expand the quantity of
sworn statements to include persons without self interest.
NO consistent rules of evidence were
applied in this case (e.g, incomplete statement from LTC Foster, NO STATEMENT
FROM BG HILL about his confrontational approach to me after I chatted with Dr
Bailey); moreover, one MAMC witness in the Provost Marshall Office who directly
contradicts Mr Cleaver's testimony, was not allowed to testify. The Command did
not allow my other witnesses to testify. These witnesses will require
guarantees from you that their careers will not be endangered if they become
known by name as my witnesses. Can you allow them to come forward with their
own testimony? This should probably not be done at MAMC. Why did BG Hill deny
my original request for change in venue to the Fort Lewis JAG Office?
#11-19
Dr O’Leary and Mr Mancuso, I can provide evidence that I did appear on
the surveillance videotapes of that day, 1 September, along with the Command
Group and the visiting dignitaries. This
contradicts Mr Cleaver's assertion that the tapes did not show any of the persons
mentioned in the hearing.
Mr Cleaver has said that he erased the
surveillance tapes of that day's events 7 days later. However, he also stated
that there were other events to be monitored that day, apart from the circumstances
covered in the hearing, requiring careful surveillance and reporting. Dr O’Leary and Mr Mancuso, I would like to ask your assistance in
retrieving ANY of the surveillance tapes for that day. If there are none, who
ordered their erasure? MEDCOM money is used to purchase and maintain this
system according to published reports from MAMC Public Affairs Office
("The Mountaineer")
#21
I reported BG Hill's remarks and actions
towards me and the threatening behavior of Mr Cleaver, as reprisal for my short
discussion with Dr Bailey. I reported this event in a sworn statement to Fort
Lewis CID. I also reported the same to MAJ Leah Cusker, the JAG officer
assigned to me by LTG Crocker.
The CID investigator told me in December
that CID did not investigate. He said that his report was forwarded to MEDCOM
for action. However, a full copy of the CID report is present within my
credentials materials at MAMC. My sworn statement predated both the statement
of Mr Cleaver and the non-signature-bearing affidavit of LTC Foster by several
months. Would this situation bear up
under usual rules of evidence?
Dr O’Leary and Mr Mancuso, which MEDCOM official did the CID report reach, and how and why
was it returned to MAMC for placement in my credentials documents?
Dr Peter Nielsen, a key witness for the
investigation of reckless endangerment
of patients at Landstuhl (1994-1996), wrote a memorandum to BG Hill's Center
Judge Advocate LTC Olmsted dated 4 December 1998. This document warned MAMC of
the impending visit of BG Kussman's investigative officer to MAMC. The officer
arrived on 6 December on a flight from Heidelberg at US Government expense to
interview me and the other witnesses regarding death and permanent injury at
Landstuhl (1994-1996).
Dr O’Leary and Mr Mancuso, quite simply stated, when I attempted to
recontact the witnesses, they were suddenly not available for questioning. Was
the investigating colonel's trip then a waste of US taxpayers' money? The
letter to BG Hill's lawyer LTC Olmsted is in my credentials records as evidence
against me. Who if anyone within the
MAMC Command prevented the witnesses from speaking with the investigating
colonel from Heidelberg? If BG Hill did not want any witnesses interviewed at
that time, could he simply not have requested a delay in the interviews from BG
Kussman? The interviews could then have been rescheduled, so that money would
not have been expended on the investigator's trip from Heidelberg to MAMC.
The credentials records under my name
appears to be a sequestering place for documents related to the Federal
investigation in Germany. This investigation was recommended in October 1997 by
LTG Blanck’s Quality Management Office in San Antonio. LTG Blanc’s travel
orders for me to brief them were instrumental in allowing the investigation to
begin.
In February of 1996, I was JCAHO
representative for Medical Staff issues reporting to COL Ney Gore, Vice
President Gore's cousin, and then COL (P) Kevin Kiley's Deputy Commander at
Landstuhl. On 12 February 1996 at 1300
hours , in the presence of Ms Michel Jung COL (P) Kiley's secretary, I reported
COL David Lipsi and LTC David Gillingham to COL (P) Kiley for reckless
endangerment of emergency patients by violation of JCAHO standards of medical
care. TWO HOURS LATER, COL Kiley
ordered my removal from his Command via psychiatric referral in violation of
DOD Directives against such reprisal actions.
Dr O’Leary and Mr Mancuso, your assistance in initiating the
investigation in October of 1997 was essential so that other patients will not
be harmed at Landstuhl and elsewhere. However, the investigation appears now to
have faltered. I believe that COL David Lipsi retired from active duty in July
1999; LTC David Gillingham was promoted and will remain on active duty. COL (P)
Kiley is now Brigadier General Kiley and reports to LTG Blanck.
Dr O’Leary and Mr Mancuso, have you determined whether the JCAHO
violations of due process which I am reporting to you in this appeal are
related to the now-faltered investigation against BG Kiley's former
subordinates at Landstuhl?
As part of the investigation which MEDCOM
authorized, I received an alarming report originating from 2 medical personnel
assigned to Landstuhl now. In November of 1998, they reported incomplete
maintenance records for 10 years previously on instrumentation used by LARMC
Ethics Committee for brain death determinations. The inability to predict the
baseline readings implied that it is possible to declare a person brain-dead
when that person is alive. I relayed the report via e-mail and verbally to the
investigator in Heidelberg.
Dr O’Leary and Mr Mancuso, Dr Nielsen's testimony was crucial to the
other case involving the LARMC Ethics Committee in 1996. Dr Nielsen declined to participate in the
investigation partly because medical records and radiology data were not
supplied to him in advance from the case of the infant who was allowed to die
of an easily correctible condition. The investigator from Heidelberg told me
that he had gone to Landstuhl in November 1998 to obtain that documentation;
however, all documentation regarding that case and others in his purview, was
unaccounted for. Dr O’Leary and Mr Mancuso,
what progress has been achieved by LTG Blanck’s office in retrieving the missing medical records
and radiologic data?
What has been the testimony of Ms Michelle
Jung, now Secretary to BG Kussman, regarding her memory of events on 12
February 1996 when I presented my complaint to then COL (P) Kiley at 1300 hours
in her presence (with a copy to her)?
Dr O’Leary and Mr Mancuso, why are my credentials records being
utilized at MAMC as a repository for documents which belong to a an
investigation in Heidelberg which was ordered by Department of the Army, based
on recommendations of MEDCOM’s Quality Management Office?
Am I correct that while I have been facing
such time-intensive skirmishes with MAMC Command regarding my own credentials,
that the investigation in Heidelberg has faltered?
Dr O’Leary and Mr Mancuso, are you going to
assure that BG Kiley of the Armt surgeon General’s, within whose sphere of
influence BG Mack Hill serves, be recused from any portion of the credentials
actions regarding me? In order for you to accomplish this, am I required to
request that he recuse himself, during official proceedings or memorandum (as during my credentials hearing
in the case of COL Jones.) Would JCAHO’s legal office be willing to assist me in preparation of such a document?
#22
Mr Cleaver reported that my uniform was
disheveled on 1 September 1998. This is disputed by the other witnesses. What
has BG Hill mentioned to you regarding this episode? What description of the
events immediately following my chat with Dr Bailey has emerged? BG Mack Hill
appeared to challenge me by name in apparent anger for my discussion with Dr
Bailey; however, BG Hill did not mention to me any problem with my uniform. How
can this be resolved without a sworn statement from BG Hill? Can such a
statement be arranged as soon as possible, so that I can receive my full
credentials back?
#26
There is a need for a sworn statement from
Ms Carole Meines to explain why I was denied access to my performance
evaluations of August, September, and October until 3 March; this was many
months too late for me to react to any constructive criticism in those
evaluations. Even more importantly, why was Dr Russell Hicks, now MAMC Chief of
Psychiatry, still considered my Army psychiatrist as shown by his continuing
reports on me to the Impaired Provider Committee from August through November
1998. And if so, why did his written evaluations of me not contain the official
report which I made to him of the episode of harassment involving BG Hill
personally, an episode which was instrumental in aggravating my clinical
depression which then caused my own self-reported lateness with records.
MAJ
Jordan appeared to indicate that the MAMC Command was preventing him
from showing me the performance reviews which he had written for my use. What
do JCAHO and AR 40-68 provide for guidance on denial of quality improvement
information for an enrollee in the impaired provider program?
#31
When I transferred to Department of
Medicine, I provided to MAJ Jordan and COL Reed complete documentation of my
Landstuhl IG report of reckless endangerment by officers reporting to then COL
(P) Kevin Kiley. The reason that I did so was that I expected the investigation
to move forward in August 1998. In the past, the demands of having to remember
the reckless incidents from Landstuhl, and the time demands of testifying by
telephone and affidavit, have diminished my capacity to work as efficiently. I
considered that both supervisors would need that information in order to help
me prevent a recurrence of major depression.
As the Germany investigation was proceeding, the events of 1 September
occurred. I reported these happenings as related to my role in the Germany
investigation, and as reprisal in violation of Whistleblower protection. And I
became increasingly depressed as I reported to both Dr Hicks and Dr Hickey, my
private psychiatrist. Dr Hicks would then be expected to report these events to
the Impaired Provider Committee under JCAHO provisions which attempt to prevent
worsening of the clinical condition for which a provider is enrolled into the
Program. In my case, depression was a very predictable outcome. Even 300 mg of
Sertraline daily and frequent appointments with Dr. Hickey were not enough to
prevent a relapse, since the time to complete late records was not given even
after due notice.
#32
Indeed, Department of the Army in August
mandated the investigation in Heidelberg into my allegations of reckless
endangerment by COL Lipsi and COL Gillingham in response to what they said were
direct orders by then COL (P) Kevin Kiley,
then-Landstuhl Commander. At the
time of Dr Bailey's visit on 1 September 1998, BG Mack Hill was in the process
of transferring to become MAMC Commander in mid-September. He had just arrived
from working in close association with BG Kevin Kiley, Assistant Surgeon
General of the Army for Force Projection.
Dr O’Leary and Mr Mancuso, what has BG Mack Hill discussed with you
about his own feelings and actions at the time that MAMC Command Group pointed
me out to him by name at the time that I was speaking to Dr Bailey about George
Washington University Medical Center, where we both trained?
#33
COL Jones
demanded that I turn in 100% of charts to MAJ Jordan within 24 hours,
according to what I remember of MAJ Jordan's comments to me. This demand was
impossible to comply with, given the increasing depressive symptoms which I was
experiencing, especially as I considered myself in danger of more episodes of
false arrest or other harassment by MAMC Command; specifically by BG Hill who
was a close associate of BG Kiley.
#34
My memoranda of 2 and 22 October addressed to COL Jones, MAJ Jordan, and COL
Reed corroborate that I was complying with the Departmental plan to bring my
records up to date as expeditiously as possible. These memorandum constitute
the “first supervisory plan” of this whole process, a plan which had the
approval of COL Reed, my Chief, as well as the clinic staff with whom I worked
daily.
#35
I kept LTC Jordan and the other Clinic
staff informed of my need for increasing frequency of psychiatry appointments. Clinic Secretary Lissette Ortiz and LTC
Jordan arranged for my replacement in the Clinic if these appointments required
me to leave during Clinic hours. I kept my clinic supervisors and the nursing
staff with whom I worked closely informed about the adverse emotional impact on my family and myself imposed by
the Germany investigations, the worry concerning them, and the time demands in
order to arrange witnesses and evidence, and to continue my patient-care
responsibilities.
#37-39
LTC Jordan and I had both discussed our
symptoms of depression with COL Russ Hicks, the Clinic's designated
psychiatrist.
#42
There is no precedent within Department of
Medicine at MAMC for permanent suspension of clinical privileges because of
record-keeping delays secondary to an episode of situational depression. BG
Hill's inaction in restoring my credentials for 8 ½ months may in fact not have any precedent within the AMEDD.
#44
Dr Hickey interpreted LTC Johnstone's
request to confirm "paranoid
delusions" as inappropriate and out of the ordinary. She knew that Dr.
Russell Hicks was my assigned Army psychiatrist, and that I had reported all of
the events to him personally twice in September 1998.
#45
Dr Hickey reported BG Hill's credentials
actions taken against me as reprisal in violation of Whistleblower Protection.
This report was furnished to COL Robert Johanson and LTC Ed Bodling of the DA
IG's office. I requested their intervention because of my fears for a
recurrence of the detention and physical assault, and my fears of MAMC's
reprisal on my credentials files. I reported this in detail to MAJ Cusker, LTG
General Crocker's JAG Officer, before she was abruptly requisitioned by BG Hill
in January 1999.
#46
The effect of BG Hill's anger directed at
me followed by Mr Cleaver's detention and physical assault, both aggravated my
depressive symptoms from 1 September 1998 onward.
#48-49
I can provide evidence that the
psychometric test was indeed placed into the written record and did not
corroborate an impaired score. This discrepant test was utilized by Ms Nancy
Greenfield, MAMC JCAHO expert, according to witnesses to place my credentials
under supervision.
With Dr Hickey's assistance, this situation
has been reported to American Psychological Association and JCAHO as an ethics
violation which may have interfered with due process. Dr O’Leary and Mr
Mancuso, have these organizations
provided you yet with their report of investigation? If so, may I request that
you supply me and my counsel with a summary of their report under Freedom of
Information Act, so that the information may be included in my credentials
records?
#50
Dr Hickey did not respond to LTC
Johnstone's request for a "paranoia" diagnosis, because she
considered the request irregular and unjustifiable.
#53
Dr Hickey corroborates no paranoia. This
is confirmed by the Independent Medical Evaluation ordered by BG Hill and
accomplished on 10 May by Dr Dunner. Dr Dunner corroborates that the events
reported in Army Times of 15 February 1999 regarding what occurred on 1
September 1998 would contribute to my depression. He recommends on the basis of
what BG Hill provided to him for documentation, that my credentials be
restored.
#54
There is an element of post traumatic
stress in my response to events at Landstuhl and the resulting investigation.
#58
There is a lack of trust in Ms Nancy
Greenfield and the Credentials Office because of the use of the psychometric
test result, now missing, in order to take adverse action on my
credentials. BG Mack Hill is on record,
within the Freedom of Information Act denial by MEDCOM FOIA office, stating
that there was NO WRITTEN REPORT BY LTC POWELL of the psychometric test. I know
that LTC Powell did in fact generate a written report of the test, because he
did so in my presence, during my followup talk with him on 4 April 1997! I can
provide for you my verbatim record of LTC Powell's analysis of the psychometric
test; my meticulously detailed notes of his comments to me, which he repeated
for me to render them word-for-word, is discrepant with the results as
summarized in the credentials documents under Ms Greenfield's purview. In
particular, LTC Powell’s report is full of references to the escalating
investigation into Brigadier General Kiley’s management at Landstuhl in the
years 1994-1996; it contains a brief timeline of events and the psychological
effects of such events.
Dr O’Leary and Mr Mancuso, the records of both the MAMC Psychiatry
Clinic and Psychology Clinic which would corroborate this, both were
unaccounted for when BG Hill referred me to Dr Dunner on 10 May 1999. COL
Victor Bell is the former Chief of Psychiatry at MAMC. The Credentials Hearing
Chairman, COL Kelley, with concurrence of LTG Crocker's JAG officer LTC
Pearson, had delegated to COL Bell on 3 March that he investigate the issue for
the Committee. What explanation can be given for the fact that those specific
records are missing, and that BG Hill has reassigned COL Bell to Alaska?
I believe that two persons still at MAMC
have knowledge of the contents of the missing records: Deputy Commander COL
Gilman, whose arrival coincided with the disappearance of the records, and Chief of Psychiatry Dr. Russell Hicks,
who discovered the records missing and reported that fact to LTC David Smith,
Chief of PAD.
#63
Dr Hickey verifies that my ability to
handle stress is improved despite, or maybe because of, the experiences of the
last few months. Dr Dunner documents that the major depression which generated
the credentials action in November, has now resolved. Both Dr Hickey and Dr
Dunner recommend restoration of my credentials and my early retirement from the
Army.
LTG Blanck’s approval of my early
retirement, as relayed to me by your Quality Management Office on 14 May, is
much appreciated. Why has BG Hill not allowed my full credentials to be
restored so that I can leave MAMC and seek civilian employment?
Dr O’Leary and Mr Mancuso, specifically why has BG Mack Hill not verified
for Washington State Medical Licensing Office that my credentials were restored
on 3 March 1999 by vote of the MAMC Credentials Committee?
#65
Dr Hickey remembers Mr Cleaver from MAMC.
She depended upon his security help if there was a psychiatric emergency. In Dr Hickey's opinion, Mr. Cleaver would
not have detained a MAMC physician and
shoved him down the escalator without a direct order from a high-ranking MAMC officer.
A review of Mr Cleaver's job description provided by the Fort Lewis Freedom of
Information Act Office confirms that Mr Cleaver would follow "higher
authorities" for such actions relating to policy. He has no independent
powers of arrest contained within his job description.
#72
Dr Hickey is not required to talk to job
supervisors of her patients without their permission. She was depending upon
Dr. Hicks, my officially assigned Army psychiatrist, to interact with my
supervisors. Why did Dr. Hicks exclude himself from this role? I believe that
the reason is the following: Dr. Hicks is already a principal witness in any
investigation into then COL (Promotable) Kiley’s infringement of my due process
rights to review of both the psychiatric hospitalization and the suspension of
credentials. Dr.Hicks may not have carried out his role as my Army psychiatrist
out of fear that his involvement might threaten his career advancement. BG
Kevin Kiley now controls career advancement for Army Medical Corps officers,
and BG Kiley oversees their credentialing.
#73
MAJ Rumph and Ernestine Russell and Donna
Hewitt of Internal Medicine confirm that I DID report myself as late with
records and in need of administrative time to bring them up-to-date.
#85
I requested software from MAJ Rumph to
help bring my charts up-to-date.
#88
MAJ Rumph in his past assignment worked
directly for BG Mack Hill, and has just been selected for an administrative
assignment within MAMC Command Group at BG Hill's direction.
#96
COL Cushner gives testimony that is
discrepant with other witnesses whom I would call, who are members of the
credentials committee. Cushner said that he did not act with COL Jones in
removing my credentials; however, this is directly contradicted by LTC
Johnstone's memoranda.
#114
Why did the Impaired Provider Committee
not meet as per standard procedure?
#132
LTC Hobbs demonstrates no familiarity at
all with identifying symptoms of depression through difficulties with medical
record keeping. He said that he was not informed that I was experiencing a severe
situational depression during the periods of his evaluations of my work.
#134
Maria Turner, RN, is mentioned in my
memorandum of 22 October 1998 as assisting with my rehabilitation from the
acute depression.
#148-151
The discrepant role of Dr Hicks is
discussed. He was still my doctor according to Impaired Provider Committee
records, however, would not comment fully on the events during the time period
in question.
Ms Nancy Greenfield refused to be my
witness. I therefore do not have an official ruling from MAMC's JCAHO expert Ms
Greenfield on the manner in which the reported errors in my credentials records
will be corrected in accordance with JCAHO guidelines.
I submitted a computer disk to the hearing
committee with my request for correction of inaccuracies in my credentials
records.
The objection was registered that there
are gross inaccuracies in my credentials records. What action has LTC Pearson,
Fort Lewis JAG, taken on my request?
Have you received such a request yet from Fort Lewis JAG?
#152
Was this accepted as an official challenge to accuracy?
Why were the memos documenting charting
plan not accepted into the hearing record?
What are the rules of relevancy?
How is LTC Pearson interpreting AR 40-68
with respect to rules of relevancy?
I believe that all Article 138 documents
(including my correspondence with the offices of the Honorable Louis Caldera
and Dr Sue Bailey should be accepted because the issues and the witnesses are
the same. Dr O’Leary and Mr Mancuso,
What is your judgment regarding this issue?
#157
The rating scheme NEVER included COL
Cushner; therefore, why did he with COL Jones remove my credentials. What is
your opinion of their actions?
Two witnesses on the Credentials Committee,
if given adequate anonymity and protection, will testify on my behalf that COL
Cushner was responding to orders by COL Jones, and excluded the Department
Chief and those on the official rating chain. JCAHO guidelines require that the
Department Chief's recommendation be considered in order for JCAHO guidelines
of due process to be fulfilled. Why did BG Hill appear to decide to the
contrary? What is your opinion on this matter?
The computer records from my previous
duties in Department of Emergency Medicine were submitted to the Committee to
show my own ideal model of record keeping which I achieved during my work in
the Emergency Department, but were not accepted by the Committee. Why not? Dr O’Leary and Mr Mancuso, in your hearing of this matter, would you be
willing to accept evidence of my job performance from before the time frame of
July 1998 which BG Hill imposed on LTC Pearson and the hearing.
#159
No evaluation was received by me. Why not?
Does this fact invalidate the credentials actions taken by BG Hill?
#172
Why did BG Hill delay his independent
medical examination of me until 10 May? Would you please request that he supply
any information on whether the missing Psychiatry and Psychology Clinic Records
have been found, or can be reconstructed? What if BG Hill cannot supply the
missing records? Dr O’Leary and Mr Mancuso,
would you be able to facilitate my calling of witnesses who are able to
reconstruct the information? Both are now civilians, and would need travel
orders to be able to testify.
#173
Only COL Kelley and Ms Meines signed the
hearing minutes. Why did LTC Pearson LTG Crocker's JAG officer not sign? Was
the document reviewed by JAG?
Enclosures
#LTC Foster's statement is included;
however, it is not properly sworn. Why not?
#Dr Bailey's letter for the Credentials
Committee of 3 March.
Was Dr. Bailey's letter not accepted as
evidence? If not, was LTC Pearson's
legal opinion stated?
#CID STATEMENT/JCAHO
How did the signed statement from Fort Lewis
CID reach my credentials file. Why was my sworn statement read during the
Credentials Hearing, while no other witnesses submitted a sworn statement
regarding the events of 1 September? Why were my JCAHO reports against then-COL
(P) Kevin Kiley allowed into the documentary portion of my Credentials Records?
Dr O’Leary and Mr Mancuso, if Fort
Lewis CID Agent Navora submitted his report to MEDCOM of the 1 September
incident, how did his report find its way into MAMC's Credentials Records under
my name? Is the CID record not a protected document under current Whistleblower
protections?
#American Psychological Association ethics
violation report, draft by Dr Hickey
The official report is on file with APA
and with JCAHO.
#Army Times, 15 February 1999, page 15,
Karen Jowers
#Bubble sheet order of 9 November 1998
Documentation of written unlawful order
which COL Cushner was directed to carry out.
I reported this during the hearing to LTC Pearson of LTG Crocker's JAG.
My evaluations from August, September, and
October from LTC Jordan to Impaired Provider Committee were entered into
evidence; however, I did not see them before 3 March, contrary to regulations.
I reported this during the hearing to LTC Pearson of LTG Crocker's JAG.
I have other legal challenges to forward
to you regarding the documents in my credentials records: however, I will
reserve these until we can review the original documents together with
attorneys present.
22 March 1999 Credential Hearing
#6
The final finding was as follows:
1. Possible actions unbecoming an officer
2. Bizarre behavior
3. Several discrepancies in testimony
4. Possible 15-6 investigation by BG Hill
Why was this language inserted into the
hearing record before BG Hill signed the record? Much of this language was not
present in previous records. Was LTC Pearson of LTG Crocker's JAG present when
the language recommending 15-6 investigation was added? Did LTG Crocker's JAG
office approve these apparent inconsistencies in the minutes? If not, why not?
If not, would you please send the record for legal review by Mr Bressler,
General Counsel for JCAHO, as well as DOD attorneys?
#7
Signatures
Col Kelley
Ms Meines
BG Hill
Why did no JAG officer sign? Did either MAJ
Cusker of LTG Crocker's JAG, or LTC Olmsted of MAMC, participate in the
additional language which was apparently added after the hearing ended?
Credentials file received 13 January 1999
#20 Page
Discussion of ad hoc minutes
My clinician Dr Williams considered the
test result normal according to his memorandum just obtained under FOIA. These
inaccuracies were reported to LTC Pearson of LTG Crocker's JAG office. What
action has been taken to correct the record?
When BG Brown withheld his signature, is
that when the psychometric test was entered into my record? If it was a normal
result, how could it have been used to call the emergency meeting to place my
credentials under supervision?
There is a confusion whether or not JCAHO
or Army Regulations were being used to consider the psychometric test abnormal,
when the numerical reading was normal. Dr O’Leary and Mr Mancuso, what is your interpretation of whether the
normal test result, called abnormal, was utilized properly under JCAHO or Army
Regulations?
The memorandum by MEDCOM which identifies
me as whistleblower accusing COL (P) Kevin Kiley of issuing orders to abandon
care of emergency patients was sent to BG Brown by Cynthia Vaughn of MEDCOM on
3 April. What was the reason that BG Brown took the credentials action which he
did utilizing a normal psychometric test? Has this had a legal review by JAG or
JCAHO.
#14
There is a discrepancy about whether JCAHO
or Army Regulations were applied here. Dr O’Leary and Mr Mancuso, what is the reason that MAMC Center JAG
ruled that his would not hold up to legal scrutiny? If, as the credentials
minutes reflect, that MAMC's own JAG was concerned about this point, what is
your decision?
#58
Hearing notice
LDr O’Leary and Mr Mancuso, did BG Hill's order to schedule the hearing
date before assigning me Trial Defense Attorneys have LTG Blanck’s approval?
Had it been staffed through LTG Crocker's JAG?
#72
Supervisory Plan
COL Cushner was never my supervisor-never
in rating chain. Who gave him authority to relieve me for cause? Did BG Hill
ask for LTG Blanck’s authority to act outside of the usual rating chain, and if
so, why? Was the Troop Commander at MAMC informed of this irregularity, and is
there a notation to that effect in my Army Personnel Record?
LEGAL CHALLENGE NOTATIONS
The following are notations of documents
and portions of documents which I intend to point out to you when you hear my
case:
#1 sept 98: where is the report of arrest?
#memos 2+22 oct to these supervisors
#secret chart review by non-superv
cushner, while I was out of
town ordered me out of my office
# 086
21 may 98
088 Health Provider Action Report
DD Form 2499 forwarded to OTSG per
Regulation
12 Sep 96 "followed continuously by
MPHP "
Dr O’Leary and Mr Mancuso, my credentials document that MAMC kept LTG
Blanck informed fully of my enrollment in the Impaired Provider Program because
of the situational major depression which I sustained at LARMC. Was LTG Blanck
informed when my Fort Lewis CID report reached MEDCOM? Was he briefed that a
physician at MAMC, enrolled in the Impaired Provider Program reported to his
office, had reported meeting Dr Bailey, Assistant Secretary of Defense for
Health Affairs on 1 September 1998.
Was LTG Blanck informed that the CID
report documented an angry approach toward me by BG Mack Hill followed by
detention and physical assault by Mr Cleaver of MAMC Security? If BG Hill did
not report this to you, CID says that they did report it. What action was
taken? I remember that LTG Blanck was
scheduled to be present that day, but was called back for an urgent
meeting with General Dennis Reimer, former Army Chief of Staff. Was General
Reimer briefed that day by LTG Crocker's office about the event.
Dr Bailey states in her letter that she
does not recall such a report at the official briefings that day. What is your
opinion? I have a more detailed report filed with MAJ Cusker of LTG Crocker's
JAG office which I will provide you with at the appropriate time.
I request that MAJ Cusker of LTG Crocker's
JAG be granted travel orders to be present for any briefing.
#97-99
Dr O’Leary and Mr Mancuso, the following notations are regarding
documents on file in BG Hill's credentials record under my name. They provide
some of the information which was in the Clinic Records under COL Bell's
purview, before the records were “unaccounted for.”
#23 February 1996
LARMC Ad Hoc Credentials Meeting
Timeline notes for future reference:
LTC Gillingham had threatened to deploy 3 out of 6 ER physicians, quoting
orders from then COL(P) Kiley.
Change in meds to resolve depression.
Situational depression is the more correct
description.
No notification of rights of due process
was ever rendered.
#99 16 Feb 96
Impaired Provider Minutes
What is evidence for delusional thinking
during a situational depression?
#Impaired Provider Referral
Ordered by then COL (P) Kevin Kiley 2
hours after the presentation of the IG complaint against COL David Lipsi and
LTC David Gillingham.
#142
Memo irreg 5 feb 96
Did LTC Gillingham not approve my clinical
privileges previously? Did COL Gore then have to write a memorandum to explain
this irregularity? Was OTSG briefed on this at the time?
#190
Why did BG Hill have the MAMC Credentials Office
call the legal offices of ALL states in which I have EVER had a medical
license, in order to check for infractions? Were you informed of this action?
Why did the Credentials Office label my California State License
"delinquent" when that certainly is not substantiated by California
State records? Were you informed of this discrepancy? What does BG Hill mean by
the term "delinquent?" Is the use of the term "delinquent"
the reason that Washington State has not yet granted me a licence, or is the
delay explained otherwise?
Abeyance 25 nov98
#216-219
Abeyance 3 Nov 98 states "lack of
medical documentation despite counseling." There WAS no counseling. What
is your opinion of the lack of signature of counseling on LTC Jordan's
counseling statement of 1 December, my lack of knowledge about the performance
evaluations that LTC Jordan had written about me to Impaired Provider
Committee, and my written statements for the record on 2 and 22 October
documenting my best effort to catch up on medical records?
How do you intend to reconcile such
deficiencies?
COL Cushner went to Col Jones without any
authority from the Department Chief COL Reed.
"Last monthly report from supervisor
showed significant decreased function." However, as I have stated,
Impaired Provider Committee evaluation reports were never shown to me so that I
could either catch up on record keeping, or take a leave of absence for
depression.
What does JCAHO rule on required feedback
to be given by Impaired Provider Programs to their enrollees? What do Army
Regulations state about required feedback to be given by supervisors to their
rated officers before they have adverse personnel actions initiated against
them? Has this had your own review?
#220-231
"delusional":
Where is the documentation of this
diagnosis?
"1 sep inappropriate":
Without a sworn statement from BG Hill and
with no mention of BG Hill or the detention with physical assault arrest.
"disheveled uniform": Where is
the evidence?
"counsel sessions documentation
completed but not signed by either LTC Jordan or LTC Smith": How could
this have been a valid counseling session?
"manic depressive/catatonic": At the hearing, I entered
the objection that these were false statements made into my credentials
records, and requested their correction. What actions has LTC Pearson LTG
Crocker's JAG taken to correct my record? Why did Nancy Greenfield, RN,
categorically refuse to correct these fasle statements.
"COL Jones' overview: October
performance review poor:" However, there was no valid counseling session
documented.
An erroneous clinic visit history is
traced: that is, there is omitted any mention of the cardiac catheterization by
a MAMC cardiologist Dr Miller and consequent referral to pulmonologist Dr
Pluss. An accurate timeline from the MAMC computer database was evidently not
utilized.
#231
Psychiatry Evaluation is requested by
Impaired Provider Chief LTC Johnstone in November 1998.
Why did BG Hill not order the Command
Directed Independent Medical Examination until 10 May 1999?
Dr O’Leary and Mr Mancuso, the following documents are also relevant
and can be made available to you and your staff:
#322 Article 138 denied by BG Hill.
Not only did BG Hill refuse to allow his
own actions of 1 September to be investigated impartially; he also arranged
transfer of my JAG counsel MAJ Cusker to his own service! In such a serious
allegation that I made against him in the letters to Dr Bailey et al (that BG
Mack Hill participated in a series of reprisals against me for talking with Dr
Bailey, including my subsequent detention and physical abuse) it certainly
conveys the appearance of impropriety that he requisitioned the one JAG officer
who was assisting me with the official complaint.
Dr O’Leary and Mr Mancuso, I had appealed to LTG Crocker, Commander of
I Corps and Fort Lewis, for JAG assistance: LTG Crocker responded to my request
IMMEDIATELY and in good faith, by assigning me MAJ Cusker.
BG Hill's actions seemed to derail LTG Crocker's good intentions by
arranging transfer of the JAG? Dr O’Leary and Mr Mancuso, this action requires your review.
What was BG Hill's fear of facing an
investigation in the nature of a 138, which is still pending at the DA level?
#329
Letter by e-mail from BG Kussman's
investigating officer
I requested help from BG Kussman's JAG
officer against reprisal from BG Hill. I documented my evidence that BG Hill's
actions are intended and timed to derail the MAMC portion of witness interviews
and evidence-gathering. I provided information that Dr Nielson's memorandum of
4 December 1998 to BG Hill's JAG predated the investigating colonel's visit by
2 days.
Dr O’Leary and Mr Mancuso, NO witnesses were available besides myself
who could verify the reckless endangerment case from Landstuhl. Yet before Dr
Nielson's notification to MAMC Command of the impending visit of the
investigator, I had arranged for 3 major witnesses to give testimony regarding
one infant death and one untreated neuro-trauma case, as well as orders to
abandon care and to deliver below standard of care, all regarding Landstuhl
Army Medical Center under Command of then COL (P) Kevin Kiley.
#455
Apr 94 reprisal memo: This memorandum was
delivered in person to COL (P) Layland 2 months before COL (P) Kiley's arrival
at Landstuhl. It concerned JCAHO violations which endangered patient care,
including ambulances without adequate airway equipment and brakes. COL Layland
recommended an initial approach to the problems.
On COL (P) Kiley's arrival as Commander, fully
expecting that he would take decisive action as COL Layland and I had agreed, I
transferred all of the information to COL (P) Kiley. LTC David Gillingham was just arriving from Madigan Army Medical
Center. COL Lipsi ordered me to alter a document for LTC Gillingham's
credentials file. Since the request
seemed irregular, I refused the order as unlawful. COL (P) Kiley then made LTC Gillingham my new Chief and
LTC Gillingham issued orders which he said originated with COL (P) Kiley for me
to suppress all adverse quality assurance reports from my Department (Emergency
Medicine.) I refused to do so on the basis of danger to patients; LTC
Gillingham and COL Lipsi then initiated reprisals against me and my ER
personnel.
We received orders to abandon care of
certain unstable ER patient who could not immediately produce valid ID cards.
Memoranda for record were generated, and we refused to carry out the reckless
orders. LTC Gillingham and COL Lipsi then increased the level of reprisal,
claiming direct orders from COL (P) Kiley.
Adverse patient outcomes were reported,
and when this information was to be presented to JCAHO, I was medically
evacuated 7,000 miles away to MAMC, where I have continued the complaint
despite what I am reporting to higher headquarters as reprisals by MAMC
Command. The investigation was finally coming to fruition in August 1998, with
the help of LTG Blanck's report to DA and the 12 point 15-6 investigation under
BG Kussman's jurisdiction.
Apparent violations of due process
regarding credentialling were initiated against me in apparent reprisal, under
the command of BG Mack Hill. My credentials are still not officially restored
by BG Hill. Meanwhile the Heidelberg investigation recommended by LTG Blanck
has faltered. COL Lipsi will retire 1 July 1999. This would not be allowed
under current DOD guidelines if COL Lipsi were truly a respondent in an
on-going investigation.
PLEASE SEE ATTACHMENTS AND THE FILES TO BE
REVIEWED IN THE PROCEEDINGS
#462
Letters to Secretary Caldera and Dr Bailey
#467
McClatchy newspaper memo
#475
LARMC witness memos
#495
Kelly Theriot article
#496
Island Packet article on neuro-trauma case
#517
Ft Myer CID report
#521
MG David Hale Article regarding
Court-martial at Fort Lewis
#522
Meines Medcom Memo
#525
Da IG Blackened out
#526
Col Jones
#528
BG Kussman
#530
Neilson Memorandum
Bubble Sheet Memo
#534
COL ALLEN RHODES MEMORANDUM (former MEDCOM
Inspector General)
From - Sat Oct 18 14:33:07 1997
Received: from DNS1.AMEDD.ARMY.MIL (DNS1.AMEDD.ARMY.MIL [192.138.80.129])
by
pol.net (8.8.5/8.8.5) with ESMTP id KAA16561
for
<stevewsmith@pol.net>; Fri, 3 Oct 1997 10:17:06 -0400 (EDT)
From:
col_allen_rhodes@medcom2.smtplink.amedd.army.mil
Received: from
medcom2.smtplink.amedd.army.mil by DNS1.AMEDD.ARMY.MIL with SMTP
(8.8.5/16.2)
id JAA25127; Fri, 3 Oct 1997 09:13:46 -0500 (CDT)
Received: from ccMail by
medcom2.smtplink.amedd.army.mil (ccMail Link to SMTP R6.00.02)
id AA875888242; Fri, 03 Oct 97 09:18:22 -0600
Message-Id:
<9710038758.AA875888242@medcom2.smtplink.amedd.army.mil>
X-Mailer: ccMail Link to SMTP R6.00.02
Date: Fri, 03 Oct 97 08:37:30 -0600
To: <stevewsmith@pol.net>,
<col_phil_savoie@medcom2.smtplink.amedd.army.mil>,
<cpt_jeanette_stone_at_medcom11__fshtx@medcom2.smtplink.amedd.army.mil>,
<ltc_stephen_smith_at_medcen4-mamc@medcom2.smtplink.amedd.army.mil>
Subject: Re[2]: OFFICIAL REPORT TO MEDCOM
JAG & TO MEDCOM CID
MIME-Version: 1.0
Content-Type: text/plain; charset=US-ASCII
Content-Transfer-Encoding: 7bit
X-Mozilla-Status: 0000
Phil-
As I am taking a day or two off, am
working this one from home. I am
disturbed, to say the least, by LTC
Smith's accusation that the
MEDCOM IG office never instigated an investigation--they
guy is
clearly a few bricks short of a load. I will provide him a reply
next week when I am in the office and have
access to my regulations
and policy documents.
His expectations and reality are not
necessarily the same.
Birds were thicker yesterday than I have
ever seen before, anytime,
anywhere.
See you Monday.
allen
_______________________ Reply Separator
_______________________
Subject: Re: OFFICIAL REPORT TO MEDCOM
JAG & TO MEDCOM CID
Author:
COL Phil Savoie at MEDCOM11_FSHTX
Date:
10/1/97 4:47 PM
Dr. Smith
As I am certain CPT Stone advised you, the MEDCOM Judge Advocate
office stands ready to assist in any investigation that is initiated
regarding your allegations. The JAG
office does not, however, have
independent investigative authority, as does the CID, IG, commanders
IAW AR 15-6 and AR 40-68 (QA focused) and members of congress. The
JAG office simply cannot initiate an investigation.
We do, however, work closely with those investigative activities and
provide legal support and advice when needed. Undoubtedly, if one of
the agencies finds evidence of wrongdoing, they will consult with my
office for advice on how to proceed further. We stand by to assist in
any way possible. You may feel
free to advise anyone who is
investigating this matter that they may consult with this office.
Philip A. Savoie
COL,JA
Staff Judge Advocate
______________________________ Reply
Separator _________________________________
Subject: OFFICIAL REPORT TO MEDCOM
JAG & TO MEDCOM CID
Author:
LTC Stephen Smith at MEDCEN4-MAMC
Date:
10/1/97 08:35
1 October 1997
COL Savoie
CPT Stone
I appreciate your participation in assisting with my report to COL
Atkinson for LTG Blanck about allegations of unlawful command activity
at my previous assignment. Your help is appreciated since, as my
witnesses reported to me on 6 September 1997, the witnesses reported
evidence of falsification of Medical Records in the neuro-surgical
case of 3 June 1995, as well as diversion of ambulance equipment from
patient care, where it was badly needed to maintain standard of care,
to apparent black market activities which CID is already
investigating.
I have reported to my Members of Congress that I requested THREE
investigations at MEDCOM last week: (1) MEDCOM QA, (2) MEDCOM JAG,
and MEDCOM CID (Agent Patrick Tangarine). Is there a case # or file # to
identify the JAG investigation? If so,
I have also reported to the Members of Congress that the MEDCOM
Inspector General investigation was NEVER initiated in regard to
interviews of any of the 65 witnesses. In fact, MEDCOM IG NEVER
interviewed me either by telephone or in person. This failure to
investigate extremely serious allegations involving a Medical Corps
LTC and a COL reporting to and following orders of the overall
Commander, a promotable COL, seems to me also a JAG and CID matter.
LRMC JAG CPT Heller also received a request to investigate on 9
February 1995; however, like LRMC IG LTC Stearns, there was a failure
to investigate.
What other information do you require in order to pursue the MEDCOM
JAG investigation of these matters?
Respectfully,
Stephen Whitlock Smith, MD
Fellow, American College of Physicians
Fellow, American College of Emergency
Physicians
LTC, MC
#536
1. Whether COL Lipsi, former Deputy
Commander, Clinical
Services, LRMC,
and LTC Gillingham, former Chief, Ambulatory Patient Care
Services, LRMC,
created a hostile work environment for the Emergency Room (ER)
staff, and
LTC Stephen W. Smith, former Chief, ER, LRMC.
2. Whether COL Lipsi and LTC Gillingham ordered LTC Smith and
other ER
physicians to violate their medical profiles.
3. Whether COL Lipsi and LTC Gillingham placed unsubstantiated
derogatory
information in the credentials of physicians at LRMC.
4. Whether COL Lipsi and LTC Gillingham improperly influenced
the
investigation of the treatment provided to ..............
5. Whether COL Lipsi and LTC Gillingham altered medical records
pertaining
to his treatment of ............. and altered ER, LRMC,
workload.
6. Whether COL Lipsi and LTC Gillingham improperly ordered
LTC Smith and
the ER staff to refuse to provide medical treatment to critically ill
and
injured German national patients technically ineligible for ER care.
7. Whether COL Lipsi and LTC Gillingham improperly conspired to
create
circumstance that would cause a bad patient outcome by exhausting
and
ruining the health of LTC Smith.
8. Whether COL Lipsi and LTC Gillingham reprised against LTC
Smith by
deliberately under- staffing the ER.
9. Whether COL Lipsi improperly threatened to refer LTC Smith to
a mental
evaluation (MHE).
10. Whether COL Lipsi improperly ordered
the opening of a fifth
operation
room while the surgical unit was critically understaffed.
11. Whether COL Lipsi improperly required ............., former
Neuro-Surgeon, LRMC, to be "on-call" 24 hours a day for 1
year.
12. Whether LTC Gillingham intentionally violated the medical
confidentially of LTC Smith's treatment for depression.
13. Whether LTC Gillingham improperly transferred 15,000
workload medical
expense performance reporting system counts from LRMC
emergency medicine
service to the LRMC primary care clinic.
LEGAL CHALLENGES BASED ON FOIA DOCUMENTS
NOTATIONS REGARDING FOIA DOCUMENTS JUST
RECEIVED
Hearing record+FOIA Documents+ 2 missing
clinic records on me
11 May 1999
#1->22
#1 cred file ->13 Jan 1999
#2 cred apart from file?none
#3 given 13 Jan 1999
**NOT**Not evals until 3 march
#2,7,13,15,19 none @ Mamc
#4 Pa names withheld
#5,8,11,12,14 enclosed
#5 psycho ltc bruce crowe
written report not generated
**I saw him generate written
report**->Ap f/u visit
#6 cred mi
**Impaired Provider**
#8 be more specific
#9
->larmc
#10 ->larmc
#16 ->jcaho denied 10 usc 1102
#17,18 jag
#20,21 not finalized by mamc cmdr
#22 tape request ->not req verbatim
transcript
#2,7j13,15,19 'no records finding'
#6,16 OTSG DENIAL
LEGAL CHALLENGES BASED ON JCAHO STANDARDS
Joint Commission
1998
Update #4
Automated CAMH
Comprehensive Accreditation Manual for
Hospitals
The Official Handbook
Accreditation Policies
Standards
Scoring
Aggregation Rules
Decision Rules
1998 Copyright JCAHO. Bound VIEWS Infobase, '98 upd #4
#39
Sentinel Event
Accreditation Watch
#40
Flow Chart
#121
Pt Rights
ethical questions
conflict resolution
reasonable access
#129
Code of Ethical Behavior
#133
implementing ethical process
#140
ethical behavior
ethical business practices
#145
Federal Crackdown on Fraud
#146
Maintaining ethical conduct throughout an
Organization
#148
internal investigation
#149
handbook for hospital ethics committees
philosopher kings
#150
gag clause
#188
h+p w/i 24h
HCFA conditions of participation
#204
'a prison plugs in'
#203
'reducing risks of phone triage'
#207
telemedicine
#208
telephone triage
#333
'a fuzzy picture'
'pathways'
#334
telemed legal slow
#337
pts respn to md mistakes
#349
SCORING AND AGGREGATION FOR
#358
SUGGESTED READINGS AND OTHER RESOURCES
#383
Hcfa conditions of participation
discharge planning
BALANCED BUDGET ACT OF 1997 (EFF 3 NOV 97)
HOME HEALTH AGENCIES (HHA)
#388
SECTION II
ORG BASED
#392
'the following is a list of all standards
for this function.'
#424
GOVERNMENT HOSPITAL
OCCUPATIONAL SAFETY AND HEALTH
ADMINISTRATION
#427
Allison mj
including dissatisfied customers on a quality
improvement team
enriches the possibilities
#436
'sentinel events'
#440
leadership
#472
radionuclides
#503
HEALTH CARE FINANCING ADMINISTRATION
#512
Env of Care
#521
Hazardous Waste
#569
Medical Equipment
#573
OSHA
#584
Human Resources
#587
HR.1 DEFINE EXPECTATIONS
#591
PEER REVIEW PROCESS
#592
*RECEIVE FEEDBACK
#588
*UNUSUAL EVENTS
#600'S
Information
#725
Governance
**#727
GO.2.2 THROUGH GO.2
*medical staff membership may be
terminated
*fair-hearing
*GO.2.3
qualified and competent CEO
*GO.2.4
compliance with applicable law +
regulation
*GO.2.5 + MS.3->MS.3.1
review bylaws + rules + reg c/w org policy
and applicable law and
other requirements
GO.2.6
*conflict resolution
GO.2.1
*conflict of interest
#730
GO.2.4
*ALL APPLICABLE LAWS+REGS
#734
*nuclear regulatory commission
#736 Management
MA.1.1 edu/exp for respons
MA.2 ceo complies w/ appl law + reg
MA.2.1 ceo prompt reg
#742 COMPLIANCE OFFICER
20.22 Medical Staff
#745
*MS.2.3.2
*fair hearing and appellate
#747
*med staff exec committee
*fair hearing
#749
*credentialing
**DOD DIRECTIVES
WHISTLEBLOWER
#749
*cred process
'range of info must be explicit'
MS.5.2
*fair hearing
(CONFLICT
(COMPLIANCE
inad ceo (Accusation 8)
*MS.5.4
*uniformly applied
*MS.5.4.4.1
*fair hearing and appeal process
*MS.5.4.5
*decisions directly related to quality of
care
#751
*MS.5.13
*DEPT CHIEF REC CONSIDERED
#757
*Intent of MS.1->MS.1.13
#775
*STANDARDS, INTENTS, AND EXAMPLES FOR
CREDENTIALING
#797
**MS.5
**'All cred files rev'd ind that thes mech
hv bn cons/unif applied
#846
Suggested readings
#965
***HCFA
REVISION TO CONDITIONS OF PARTICIPATION
LEGAL CHALLENGES EXTRACTED FROM AR 15-6
1.4.D Concurrent investigations
'procedures under this regulation do nut
hinder or interfere w/ a concurrent inv dir'd by higher HQ.'
1.7 Respondents
(designated only in formal investigations)
1.8 notify
respondent in writing
2.0 Resp
of App Authority
2.1.C Who appointed?
Senior to respondents x military
exigencies.
2.2 Admin Support
*necess facilities, etc
?contract reporter
2.3.B Legal review
servicing JA
2.3.C Effect of errors
(1) Harmless
errors
(3) Substantial
errors->nullity
material effect on an individual's
substantial rights,
(d) In
case of an error that cannot be corrected otherwise, the app auth may set aside
all findings
· >rec new inv off
(4) Failure
to object
3.SECTION-I
Conduct of the Investigation
Subtopics
Challenges/rules of
evidence/Witnesses/Commo w/ the App Auth
3.1.A Requirement
'swearing of witnesses'
3.2 Challenges
lack of partiality
3.6.A General
a-General
rules of evidence
mind of reasonable persons
3.6.C Limitations
Privileged commos
(5) Ordering
witnesses to testify (self-incrim UCMJ, Art 31) 5th Amendment
(d) read
rights under Art 31
3.7.A General
(1) no
authority to subpoena
b. Expert witnesses
3.7.C testimony & statements
3.7.D discussion of evidence
3.8
*Commo w/ App Auth
enlarging
3.SECTION-II Findings/rec
3.9 Findings
f.Expl by invest off of any irreg
3.15 Exh
b. Real evidence
**disposal per AR 190-22
3.15.E Objections.
Noted in proceedings
5.1.D legal advisor
respondent & counsel must be present
when legal advice provided to
board
5.3.A Before a session
(6)all approp records
5.3.C after proceedings
prompt prepn of proceedings
5.7. Challenges for cause
5.8.A Rights of respondent
a. Right to be present
LEGAL CHALLENGES EXTRACTED FROM AR 40-68
** upon report of recovery
impaired provider ad hoc committee req
& review statements from a physician.
1.7 confidentiality statute
(4) provides immunity
good faith
rev med QA records
1.7. E Exceptions to nondisclosure
**(1) agency
accreditation
**(2) adm/jud by dod practiioner
**(3) Gov boards, agencies, orgs to
lic/cred/mon prof stds
**(6)(criminal investigators)
**(7) protect publ health/safety
1.7.F Sec Disc
**1.7.J
FOIA
INITIAL DENIAL AUTHORITY
OTSG
2.1.B Cred committee
b.
**recs sent to Medcom for approval
2.3 Impaired provider ad hoc committee
**g.
members receive appropriate training to
assume the responsibilities of the committee.
4.1 General
a...,**The privileging process
is directed solely & specifically to
the provision of quality pt care
is not a disciplinary or pers mng mech.
4.2.B
priv acts
b.
4.4.A Military
**a.(1) elim under AR 635-100 or Ar
135-175
4.9 Suspension
(3)
QA Inv
**(a) In cases of summary action there
will be an immediate investigation. The
chairperson of the cred comm will appoint an officer, pursuant to the authority
of this reg, to conduct an informal invest and report to cred comm.
(3) Collateral
actions
**suspected drug
memb imp prov com apptd to hearing com
(2) A susp period will not ordin exceed 60
days & can only be ext by
cmdr for good cause
f. Hearing committee procedures
(3) practitioner
free to consult w/ legal counse4..
May attend....not allowed to participate.
(5) If
crim misc susp
chair adv of rights using DA Form 3881
**Any objections made by pract ruled on by
chairperson
4.9.G Action on hearing recomendations
**(2) Prior to action by cmdr recorp, incl
findings and rec, will be reviewed by a JAG or DA civ att for legal suff/not
CJA.
**3)Cmdr review
Cmdr decision
Written notice of deciio and date deliv
will be delivered to practitioner.
If restn->appeal rights
*4.9.Kk. Reporting reqs
susp->cmdr DD Form 2499
Health Care Provider Advers9 Clin Priv
Ac7io rep
RCS DD-HACAR)1611
*one copy w/i 3 d
thru nxt higher hq
to HQDA
(b) If allegn not subst
cmd will send a report w/i
7 workdays of compltn inv
to HQDA
1. Summ of info giving rise to inv
2. Rationale for cmdr's decision.
3. Notation
signifying level of confidence in practnr'5 performance
(c) Status reports (status changes) using
DD FORM 2499 until final action completed.
Form 2499
have date mailed from MTF in the top rt
corner.
(3) Hearing decision
Copies of written notice of cmdr's decision
(g above) will be sent to
the next hhq
(4)**Restn
DD Form 2499
submitted per (1) above
(5) Rep actns unprof conduct.
DD Form 2499per (1)
(a)fraud/(b)fraudcontract/(c)cheating/(d)serious
misdemeanor/(e)nolo
contendere/(f) abr prof res
**(6)Charged practitioner sepn
until crim invs & res priv action
final
**UNLESS SEC ARMY authorizes earlier sepn.
**(7)Reporting authority=TSG
***FOIA INIT DENIAL AUTHORITY
FED ST MD BDS
NAT PRAC DB
OTHER APPR CENTR CLEARING HOUSES
(8)
Late charges
**12 months after sepn
**DD Form 2499
***4.10
Appeal process
OTSG
(HQDA (SGPS-PSQ), 5109 Leesburg Pike,
Falls Church, VA 22041-3258
CERT MAIL RET/REC/REQ
4.11 Practitioner's
credentials file
a.PCF
**DOCUMENTS
SIX PART FILE
(1) I
a. Id photo
b. Da f 4691-R
c. Da f 5440-R series (current and past)
d. Da f 5441-R series (current and past)
e. Da f 4692-R clin priv ann eval (past)
f. Da f 5753-R USAR for RC
II
a. Da f 5374-R (current and past)
b. Prov act prof data per
4-8e(3)
c. Cred/priv granted from civ mtf's
(3)
III
Documents of adv actn
a) Letrs of notif
b) Letrs of ack
c) Hearing summary or minute
*d) Investigations
e) Adv stm to include NPDB reports
f) Letters of decision
g) Mal claims
NPDB
h) Copies of any other adverse infm
IV
a. Cme
b. Lectures
(5)
Sec V
Da forms frum preu mtf's
(6)
Sec VI
a. Dipl/lic
b. Verif para 4-6 c
B. Pcf release only
c. Pcf kept for career
d. PCF forwarded
e. Disp pcf
(1) pcf/paf w/ p
Ar 40-68 cont
(1) Hqda at sepn
(2) pcf stays 12 months at mtf
(3) pcf if sep/ret-> Ar 25-400-2, fn 40-66d
4.12 PAF
a. Peer rev working file
(1) Practice profice AQCESS practice
profile reports:
dc's, proc./deliv/icu/deaths
(2) ave daily pt load/#times emerg
suc/deployed/supvr
AR 40-48
(3) Outcome
numb cases subst
(4) MALPR
**(5) Adm
**(6) Committee Actions
(7) Other
4.13 NPDB
REPORTS
**Pl 99-660
NPDB
HCP DATA BANK INQ
(HEALTH CARE QUAL IMP ACT of 1986 PL
99-660, title IV
'HCP (para 9-1) reported
10 USC 1102 protection
unless info false
4.13.C Prof rev actions
**c. Prof rev actns (TSG notif auth)
(1) adv priv
(2) unprof conduct
(3)
4.13.D
PCF
d. For
NPDB placed in Part III
4.13.E
NPDB Reports to nxt higher HQ TO
***TSG
***copy given to HCP**
**Inq made
**by Medcen at beginning of inv of HCP for
subst perf or unprof behav
**7.2
Obj of Imp Prov Prog
a. Prev
imp and promote well-being ...minim factors that contribute to impairment
b. Id
imp asap in order to promote recov & ensure pt safety
d. Prov
mech for returw to clin prac for HCP's who have been successf rehab
e. Prov
a mech for ongoing monitoring
7.3 Mnmnt imp by med/psych
a. Any hcp KNOWN OF having Psych
rep to imp prov ad hoc comm
(para 2-3)
c. Imp Prov ad hoc comm
will review
e-Upon report of recovery
rec to cred comm re removal of limitations
7.4.B
Imp prov rep
b. Imp
prov susp of drug abuse
rep to Imp Prov Ad Hoc Comm
**7.4.C Program Compon
c. AR
600-85
(1) Prevention
7.5**Notif to prof reg auth
a. Per
para 4-9k for privileged
b. Notif
for any HCP who
(1) susp/lim/restr/revoked
(2) illegal
drugs
(3) separates
in less than full practice
(4) leaves
w/i 2 yr monitoring
9.0 Prof Lic
**Ar 600-8-2
Susp fav pers actions
OTHER REFERENCES TO WHICH WE SHALL REFER
AT THE HEARING
References
1. 1993 Accreditation Manual for
Hospitals, volume I. Standards. 1992 by the Joint Commission on
Accreditation of Healthcare Organizations.
One Renaissance Blvd, Oakbrook Terrace, IL 60181.
2. 1993 Accreditation Manual for
Hospitals, volume II. Scoring
Guidelines. 1992 by the Joint
Commission on Accreditation of Healthcare Organizations. One Renaissance Blvd, Oakbrook Terrace, IL
60181.
3. USAREUR Regulation 632-10, paragraph
26a:
"Personnel will not interfere with,
or prevent any person from presenting, a complaint or grievance, real or
imagined, to the person's superior, commanding officer, Member of Congress, or
other appropriate agency."
4. US P.L. 102-484, Sec 546: Mental Health
Evaluations of Members of the Armed Forces.
LEGAL PRECEDENTS
VOGE
KIRKLAND
TUFARIELLO
PEARL
WALLENBERG
WEISS
REID
REIMAN
NORRIS
SCHALLER
Dr O’Leary and Mr Mancuso, my counsel and I have other legal challenges
to forward to you regarding the original documents in my credentials records:
however, I will reserve these until we can review the original documents
together with JAG and other counsel and a recorder present.
PLEASE SEE ATTACHMENTS AND THE FILES TO BE
REVIEWED IN THE PROCEEDINGS
Honorable Louis Caldera
Secretary of the Army
101 Army Pentagon
Washington, DC 20310-0101
SUBJECT: REQUEST
FOR AN INVESTIGATION IN THE NATURE OF AN
ARTICLE 138 INVESTIGATION
Dear Sir:
I am an active duty Army Lieutenant
Colonel and a doubly board-certified physician currently assigned to Madigan
Army Medical Center in Tacoma, Washington. I urgently request that you initiate
an investigation, in the nature of an investigation under Article 138 of the
Uniform Code of Military Justice, and that the subjects of the investigation
include, but not be limited to, Brigadier General George Brown, Commander of
Madigan Army Medical Center, and of Brigadier General Kevin Kiley, former
Commander of Landstuhl Army Medical Center and currently assigned to the Office
of the Surgeon General of the Army.
In February 1996, when I was assigned to
Landstuhl Army Medical Center in Germany, I requested an Inspector General and
Congressional investigation of allegations of wrongdoing by certain high
ranking Army doctors at Landstuhl. General (then Colonel) Kiley was
specifically aware that I had initiated the complaint, which concerned allegations
of intentional reckless endangerment of emergency patients at Landstuhl by two
physicians who said they were following General Kiley's orders.
In my view, General Kiley's Inspector
General at Landstuhl, LTC Stearns, failed to undertake an adequate investigation
of the allegations. When I continued to pursue the complaints and press for an
investigation in February 1996, the response included (1) medically unjustified incarceration in a locked psychiatric
ward at Madigan Army Medical Center, then and now under the command of BG
Brown; (2) orders, against Army Regulations, to move my family from Landstuhl
to Madigan immediately (even with two school-aged children) (3) explicit
threats to remove my medical credentials after the Army Times began making inquiries
about General Kiley, (4) explicit threats by the Command in early 1998 to
reduce my credentialing status to that of a General Medical Officer (one who
has not completed residency training), and (5) most recently, unjustifiable
detention by General Brown's civilian chief of security who told me he was
acting under instructions from the Command.
Selected documentation concerning this
matter is attached, consists of (1) a
lengthy, detailed letter to the editor dated May 11, 1998, concerning the events
at Landstuhl and my efforts to get them investigated and (2) a July 28, 1998, article from the Hilton
Head (South Carolina) Island Packet about one of the tragic events at Landstuhl
referred to in my May 11, 1998 letter to the editor. There is already some
press awareness of and interest in the allegations concerning Landstuhl Army
Medical Center.
Sir, should you so direct, I am prepared
to brief you or your representative regarding this serious complaint. My duty
telephone number at Madigan Army Medical Center is: (253) 968-3866. Before
other patients are harmed, I request an immediate investigation regarding the
now long-reported actions and related orders of BG Kiley, COL Lipsi, and LTC
Gillingham at LARMC, as well as the resulting coverup. In accordance with
Section 846 (Safeguarding of military whistleblowers) of Public Law No.
100-456, otherwise known as the Boxer-McDermott Whistleblower Protection Law, I
continue to request career protection from appropriate Members of Congress in
keeping with the law's intent to protect military whistleblowers from
retaliation.
In order to brief yourself or other
officials high in the chain of command in Washington, DC, I would require
military travel orders to be released from my patient care responsibilities
long enough to give a thorough testimony regarding these extremely serious
allegations.
Thank you for your attention,
STEPHEN WHITLOCK SMITH, MD, LTC, MC
(GEORGE WASHINGTON UNIVERSITY, 1980)
Fellow, American College Emergency
Physicians (1990)
Fellow, American College Of Physicians
(1983)
Cc: Rep. Dicks, McDermott, Pelosi, Spence,
Sen. Boxer, Feinstein, and Thurmond, For Record
Honorable Sue Bailey, MD
Assistant Secretary of Defense (Health Affairs)
1000 Defense Pentagon
Washington, DC 20301-1000
RE: Our Discussion at Madigan Army Medical
Center on the Occasion of
the Ribbon Cutting Ceremony for TriCare
Senior Prime, 1 September 1998
Dear Dr Bailey:
It was a great pleasure to make your acquaintance
as another graduate of George Washington University School of Medicine. I have
very fond and valuable memories of our school, and about what I learned there
about the patient's welfare coming first before all other priorities.
As you may recall, when you were recently
at Madigan Army Medical Center, we talked briefly in front of the Internal
Medicine Clinic where I am the Acute Care Physician for Medicare Internal
Medicine patients. As we discussed, I had hoped to participate in guiding your
tour through our clinic, particularly since Internal Medicine has signed up the
majority of the new Medicare enrollees.
After my conversation with you, however,
Brigadier General (BG) Brown's civilian personal security chief detained me and
escorted me away from your tour. He physically obstructed my access to the
first floor of the medical center; coerced me with a hand at my back and waist;
and escorted me to his office on the second floor. I was astonished when he
said that the Command (or Commander, (I did not hear distinctly which of the
two titles he used) had accused me of being a security threat to you; that I
was accused of carrying a concealed weapon; and that he might have to "pad
me down" for weapons. I had nothing of the kind in my possession, do not
own a weapon, and, even if I did, would never bring a weapon to work. I offered
to allow him to search me; however, he did not do so. He finished the
interrogation by telling me that the Command ordered me to return to my duty
station, and that my Department Chief was directed to lead your tour through
Internal Medicine's new TriCare Senior Prime Clinic instead of myself. He
escorted me, again physically restraining me with a hand behind my waist, down
two escalator flights, well away from BG Brown's conference room where your
afternoon tour was to begin. Rather than make an inappropriate scene, I
remained quietly in the Internal Medicine TriCare Senior Prime Clinic where I
am assigned as the Acute Care Physician. Your tour never entered our section.
I'm not absolutely certain why the
General's security chief took this extraordinary action, but, given that I am
the source of an official complaint, currently being investigated, about
alleged wrongdoing by several high-ranking Army physicians, I have to wonder if
the purpose was to limit my contact with you lest I take the opportunity to
discuss the complaint and related investigation to you.
I respectfully request and would
appreciate an opportunity to discuss this situation with you, at your earliest
convenience.
I am requesting today that the Secretary
of the Army initiate an investigation, in the nature of an investigation under
Article 138 of the Uniform Code of Military Justice, to determine what actions
BG Brown instructed his civilian security chief to take against me, the reasons
for such actions, and whether such actions improperly restricted me from having
access to you to discuss my pending complaint of wrongdoing by high ranking
Army doctors which I observed at Landstuhl Army Medical Center when I was
assigned there before coming to Madigan Army Medical Center. As BG Brown knows
well, I have not been silent about what happened at Landstuhl and I frankly
believe that certain actions taken against me at Madigan were reprisals for my
refusal to keep quiet about the events at Landstuhl which are the subject of my
complaint.
Selected documentation concerning this
matter is attached, consists of (1) a
lengthy, detailed letter to the editor dated May 11, 1998, concerning the
events at Landstuhl and my efforts to get them investigated and (2) a July 28, 1998, article from the Hilton
Head (South Carolina) Island Packet about one of the tragic events at Landstuhl
referred to in my May 11, 1998 letter to the editor. There is already some
press awareness of and interest in the allegations concerning Landstuhl Army
Medical Center.
Dr Bailey, should you so direct, I am
prepared to brief you regarding this serious complaint. My duty telephone
number at Madigan Army Medical Center is: (253) 968-3866. Before other patients
are harmed, I request an immediate investigation regarding the now
long-reported actions and related orders of BG Kiley, COL Lipsi, and LTC
Gillingham at LARMC, as well as the resulting coverup. In accordance with
Section 846 (Safeguarding of military whistleblowers) of Public Law No.
100-456, otherwise known as the Boxer-McDermott Whistleblower Protection Law, I
continue to request career protection from appropriate Members of Congress in
keeping with the law's intent to protect military whistleblowers from
retaliation.
In order to brief yourself or other
officials high in the chain of command in Washington, DC, I would require
military travel orders to be released from my patient care responsibilities
long enough to give a thorough testimony regarding these extremely serious
allegations.
Thank you for your attention,
STEPHEN WHITLOCK SMITH, MD, LTC, MC
(GEORGE WASHINGTON UNIVERSITY, 1980)
Fellow, American College Emergency
Physicians (1990)
Fellow, American College Of Physicians
(1983)
Cc: Rep. Dicks, McDermott, Pelosi, Spence,
Sen. Boxer, Feinstein, and Thurmond, For Record
(From HILTON HEAD ISLAND PACKET, McClatchy
Company)
Header: Category: Local News, Creator: Mike
Ramsey, PaperDate: 7/28/98, PaperPage/Section: 1A, End of Header.
BY MIKE RAMSEY Packet staff writer
Bobby Wood was an experienced off-road
cyclist, an "A" student and computer whiz when a bicycle wreck three
years ago sent him into a coma and changed his life. Wood, now 20 and living on
Hilton Head Island, still rides his bike every day and has been taking design
courses at Savannah College of Art and Design. But it¹s not the life he
planned. He suffered brain damage, as well as loss of vision and some mobility,
and he canceled his plans to attend Rochester University on a $32,000
scholarship.
Worse, Wood and his family contend the
damage might have been prevented had he received proper care at a U.S. military
hospital in Germany, where Wood was living when the accident happened.
"I¹m angry, but what can I do?" Wood said. "They know they have
done something wrong, but won¹t do anything about it."
Wood has filed a claim against the U.S.
Army for malpractice, but he and his family aren¹t optimistic. The Army¹s
Office of the Judge Advocate General in March turned down Wood¹s initial claim
for $7.5 million. Wood¹s attorney filed an appeal and the results of the appeal
should be back in a few weeks.
If the appeal is denied, Wood has no
recourse, said Pamela Brem, an attorney working for Wood. The case has
attracted the attention of U.S. Sen. Strom Thurmond, R-S.C., chairman of the
Senate Armed Services Committee. Thurmond has ordered an inquiry into whether
the Army¹s review of the case was thorough and above-board.
John DeCrosta, Thurmond¹s press secretary,
said it probably would take several months before any investigation results
would be available. Wood was 17 years old in June 1995 when he fell off his
bike and hit his head. He knows he was knocked unconscious, but does not know
for how long. Wood¹s mother, Nohy Wood, took him to the closest hospital,
Landstuhl Regional Medical Center, a military hospital.
It was a holiday weekend in Germany, and
no local doctors were available, she said. Landstuhl¹s emergency-room doctor
sent Wood home after treating him for scrapes and bruises, according to Wood¹s
claim. The doctor didn¹t admit Wood for observation or perform a CT scan.
The next day, Wood started bleeding inside
his skull, cutting off oxygen to his brain, according to the claim. When Wood¹s
parents took him back to the hospital, there was no neurosurgeon at the
hospital to perform surgery. Wood had to be taken to another hospital, delaying
surgery by 70 minutes, the claim states. He stayed in a coma for two weeks and
suffered brain damage.
Wood maintains that the emergency room
doctor the first day should have admitted him to the hospital for observation
and performed a CT scan. That would be standard procedure for anyone who lost
consciousness for more than 30 seconds.
Legal hurdles, i.e. Wood¹s legal battle
with the Army is made even more difficult because claims against the military
are handled differently than other types of civil claims. Brem said a division
of the Army, called the Office of the Inspector General, investigates claims
against the Army.
In addition, Army officers investigate and
decide the claims. If they deny a claim, a victim can appeal the decision to
federal court and go before an independent judge and jury. But if the incident
occurs overseas, the process stops with the Army.
"It¹s a good faith system," Brem
said. "Potentially, the Army could come back and say, Yes, we were
negligent, but we still aren¹t going to award you damages." Another lawyer
working on Wood¹s case, Richard Weiss of Boston, said he may file a lawsuit in
federal court accusing the Army investigators of "not acting in good
faith." He said facts had been ignored or unaddressed in the Army¹s
denial.
"Self-regulation doesn¹t work on any
level," Brem said. "One of the reasons doctors here work so hard to
maintain high standards is the fear of malpractice. Doctors at the (military)
hospitals overseas don¹t worry because they know people can¹t touch them."
The lawsuit could end up in the U.S. Supreme Court, Brem said. Similar
lawsuits, which attack the law governing this case have been challenged, but
upheld by the Supreme Court. Dr. Stephen Smith, the former emergency room chief
who saw Wood on his second visit to the hospital, has filed a series of
complaints against the leadership at Landstuhl, citing Wood¹s treatment as one
example of a number of problems.
Despite what Brem calls "extremely
substantial" evidence supporting Wood¹s claim, neither she nor Weiss are
optimistic about winning the appeal. Weiss claimed in the appeal that the Army
investigator, Maj. Douglas Dribben, "misstated or distorted facts" in
the case. Neither Dribben nor any other official in the Army Claims Service
could be reached for comment.
In turning down the claim, the Army
investigators said his parents should have brought him back to the hospital
earlier, when Wood experienced shooting pain in his head. And the denial states
that a CT scan the first day would not have revealed the bleeding in Wood¹s
head because it didn¹t start until the next day. But Smith said that wasn¹t
necessarily true, and the doctor should have held the boy overnight anyway for
observation because Wood had lost consciousness during the fall.
Author:
LTC Stephen Smith at MEDCEN4-MAMC
Date:
9/18/97 11:24 AM
Priority: Normal
Receipt Requested
TO: LTC Darrell Stafford
TO: COL Sid Atkinson at MEDCOM3_FSHTX
TO: COL James Kirkpatrick at MEDCOM5_FSHTX
TO: LTC Ann Brazil at MEDCOM3_FSHTX
TO: Charles Deal at MEDCOM3_FSHTX
TO: Karyn Del Rio at MEDCOM3_FSHTX
TO: Andrea Shea at MEDCEN3_MAMC
TO: COL Matthew Rice at MEDCEN1_MAMC
TO: Michael Meines at MEDCEN1_MAMC
TO: COL Casey Jones at MEDCEN1_MAMC
TO: BG George Brown at MEDCEN1_MAMC
TO: LTG
Ronald Blanck at OTSG5_FLSCHRCH
TO: BG John S Parker at OTSG1_FLSCHRCH
Subject: Re[3]: REPORT TO MEDCOM QA
STARTING 22 SEPTEMBER (NEXT MONDA
------------------------------- Message
Contents -------------------------------
Thursday, 1100 hours
I am very grateful for all of the
assistance which
you are providing to enable my report to
the
Quality Assurance experts at MEDCOM.
I have just talked with LTC Ann Brazil of
your office
who is initiating travel orders.
Special thanks are due to LTG Blanck and
Brigadier General Brown
and their staffs.
Respectfully,
Stephen Whitlock Smith, MD
LTC, MC
FACEP, FACP
per Senators Feinstein/Glenn/Thurmond
PL100-456
______________________________ Reply
Separator _________________________________
Subject: Re[2]: REPORT TO MEDCOM QA
STARTING 22 SEPTEMBER (NEXT MONDA
Author:
LTC Darrell Stafford at MEDCEN4-MAMC
Date:
9/18/97 9:46 AM
Dr. Smith: Please contact LTC
Brazil at DSN 471-6195 on your travel
plans. I just spoke with her and
they cannot see you on 23 Sep, but
can see you on 24 Sep. Please
call her or Charles Deal and they will
make the arrangements. DES
______________________________ Reply
Separator _________________________________
Subject: Re: REPORT TO MEDCOM QA STARTING
22 SEPTEMBER (NEXT MONDAY)
Author:
LTC Stephen Smith at MEDCEN4-MAMC
Date:
9/17/97 6:14 PM
17 SEPTEMBER 1997 1430 HOURS
LTC STAFFORD:
I AM NOTIFYING YOU THAT I GRATEFULLY ACCEPT LTG BLANCK'S OFFER FOR TDY
TO DISCUSS QA CONCERNS WITH MEDCOM.
THE ONLY TIME FREE FOR ME TO LEAVE THE DEPARTMENT IS NEXT WEEK, AND I
AM SORRY FOR THE LATE NOTIFICATION. I REQUEST THE FOLLOWING IF AT ALL
POSSIBLE:
1. TRAVEL STARTING MONDAY 22 SEPTEMBER IN THE
AFTERNOON
(SO THAT I CAN WORK HERE DURING THE DAY)
2. A MEETING WITH MEDCOM QA IN THE LATE
AFTERNOON
TUESDAY 23 SEPTEMBER.
MY DEPARTMENT CHIEF AND ADMINISTRATOR HAVE BEEN INFORMED AND ARE IN
AGREEMENT.
RESPECTFULLY,
STEPPHEN WHITLOCK SMITH, LTC, MC
Author:
LTC Stephen Smith at MEDCEN4-MAMC
Date:
9/18/97 12:45 PM
Priority: Normal
Receipt Requested
TO: stevewsmith@pol.net at Internet-Mail
TO: llamer@pop.flash.net at Internet-Mail
TO: lyancey@pol.net at Internet-Mail
TO: cbottoni@aol.com at Internet-Mail
TO: hasket@gwsmtp.mgmc.af.mil at Internet-Mail
TO: RTabach123@aol.com at Internet-Mail
TO: wwmed@pop.mindspring.com at
Internet-Mail
Subject: POC's and Summary
------------------------------- Message
Contents -------------------------------
Because time is short before the appointment that I have with MEDCOM,
I am sending information and POC's as available.
Author: LTC Stephen Smith at
MEDCEN4-MAMC
Date: 9/18/97 11:24 AM
Priority: Normal
Receipt Requested
TO: LTC Darrell Stafford
TO: COL Sid Atkinson at MEDCOM3_FSHTX
TO: COL James Kirkpatrick at MEDCOM5_FSHTX
TO: LTC Ann Brazil at MEDCOM3_FSHTX
TO: Charles Deal at MEDCOM3_FSHTX
TO: Karyn Del Rio at MEDCOM3_FSHTX
TO: Andrea Shea at MEDCEN3_MAMC
TO: COL Matthew Rice at MEDCEN1_MAMC
TO: Michael Meines at MEDCEN1_MAMC
TO: COL Casey Jones at MEDCEN1_MAMC
TO: BG George Brown at MEDCEN1_MAMC
TO: LTG Ronald Blanck at OTSG5_FLSCHRCH
TO: BG John S Parker at OTSG1_FLSCHRCH
Subject: Re[3]: REPORT TO MEDCOM QA STARTING 22 SEPTEMBER (NEXT MONDA
------------------------------- Message Contents
-------------------------------
Thursday, 1100 hours
I am very grateful for all of the assistance which
you are providing to enable my report to the
Quality Assurance experts at MEDCOM.
I have just talked with LTC Ann Brazil of your office
who is initiating travel orders.
Special thanks are due to LTG Blanck and Brigadier General Brown
and their staffs.
Respectfully,
Stephen Whitlock Smith, MD
LTC, MC
FACEP, FACP
per Senators Feinstein/Glenn/Thurmond PL100-456
______________________________ Reply Separator __
A SUMMARY
The precipitous drawdown of the Army's
training and quality of life
is, according to recent reports, also impacting adversely on
healthcare delivery. A number of unresolved Inspector General and
congressional cases, initiated both by patients and by Army physicians
and nursing staff are setting off alarm bells in the halls of
Congress. Multiple extremely serious allegations regarding risks to
patients and staff at the Army Medical Center level have reportedly
been bogged down at various IG levels for well over a year. Members of
Congress have still not succeeded in convincing the DA IG to conduct
interviews under oath of many key witnesses.
Recent critical attention has focussed on the US military's ONLY
Medical Center in
Europe, Landstuhl Regional Medical Center. Since Landstuhl began
transforming into the one Medical Center in 1994 and received
casualties from both Somalia and Bosnia, expectations of its level of
care have increased. Landstuhl has gained an in-patient psychiatric
unit, as well as a high risk Labor and Delivery Unit and Neonatal
Intensive Care Unit. The Intensive Care Unit has upgraded its
technology.
In 1995, a former OB-GYN service chief at Landstuhl had reported
via the Command a former Landstuhl Deputy Commander for Clinical
Services for reckless endangerment of patients and staff, and for
unlawful orders. The key precipitant of this struggle was the alleged
refusal of the former DCCS to ask for additional OB-GYN physicians to
reinforce the newly designated high risk Labor and Delivery Unit at
the beginning of Summer 1994. The written complaint alleges that only
three OB-GYN physicians remained at Landstuhl in the late spring of
1994, and that this was not enough staff for the safety of high-risk
patients. The recommendations of the Army Surgeon General's Obstetrics
Consultant were not observed, continues the allegation.
The same Obstetrics Chief also reports that when he himself succumbed
to the staff burnout which had been predicted, that the same DCCS
harassed him repeatedly over the next year, first threatening and then
actually issuing abysmally poor evaluations when the obstetrician
refused to work beyond the medical profile designed to protect him
from another major depression.
The fundamental question is not whether, but rather HOW MUCH the
quality of patient care deteriorates when physicians and nurses are
deliberately worked beyond their physical and mental capacities. An
even more dangerous situation involving deteriorating standards of
emergency care is portrayed in the stalled IG complaint of a former
Landstuhl Emergency Medical Service chief.
Informed sources report that LTC Stephen W. Smith former LRMC ER
chief presented an IG complaint to LRMC ASST IG MAJ O'Leary & to GEN
Kiley in early February 1996. This IG complaint accused COL Lipsi,
former DCCS, & LTC Gillingham, Chief of Ambulatory Patient Care, who
worked for him, of recklessly endangering LRMC ER patients, nursing
staff & physicians by unlawful orders, harassment, & disregard
of
regulations.
The complaint alleges that COL Lipsi and LTC Gillingham strictly
enforced a policy of withholding medical care from medically unstable
patients who could not prove their eligibility for LRMC services.
Whenever challenged on the basis of safety, both COL Lipsi and LTC
Gillingham reportedly affirmed that it was GEN Kiley 's order to place
unstable patients back in their cars and to advise them to go to the
nearest German hospital.
Allegedly, COL Lipsi repeatedly quoted General Kiley as ordering
that the ER RECEPTIONISTS (who are not credentialed in medical triage)
stop potentially noneligible patients at the front desk. (Emergency
medicine sources report that the standard of care is that unstable
patients are NEVER asked for their ID if there is an immediate threat
to life and limb.) LTC Smith and
the ER Nursing Staff reportedly asked
COL Lipsi for a written order that would explain hospital policy in
this regard; COL Lipsi allegedly never confirmed these orders in
writing; however, MAJOR Charles Oliver of Patient Administration
Division is credited with supplying copies of two existing regulations
which allowed lifesaving treatment until a safe transfer could be made:
"Update AR 40-3: 4-59 (1993
Edition). Civilians in emergency:
a. Any person is authorized care in an emergency to
prevent
undue suffering or loss of life. Civilian emergency patients not
authorized Army MTF services will be treated only during the period of
the emergency. Action will be taken to dispose of such patients as soon
as the emergency period ends."
"LARMC PAM 40-24: ADMINISTRATIVE HANDBOOK FOR PHYSICIANS:
ELIGIBILITY FOR MEDICAL CARE (1993 Edition)
page 16 b. In the case of US civilians visiting
soldiers In
Europe, the LARMC Commander's policy is that emergencies will be seen
immediately, and non-emergencies will be seen on a pre-paid, space
available basis when the provider determines that care is necessary to
prevent undue suffering, to include the mental suffering of attempting
to secure health care in a foreign environment. However, care will be
limited to the acute minifestation only and will not include elective
procedures or inpatient care which can be safely deferred until the
patient returns to the US."
The complaint continues that LTC Smith, MAJ Laurie Sandstrom,
former LRMC ER Head Nurse, and COL Carolyn Bulliner, Deputy Commander
for Nursing, protected the ER
receptionists from COL Lipsi's unlawful
order to practice economic triage.
Reference to a copy of the IG
report provided to Members of Congress shows the following case
summaries:
Specific Cases:
CASE #1: April 1994, 35 year old Polish female immigrant with unstable
ectopic pregancy - COL Lipsi allegedly ordered both Er physicians CPT
Anderson and LTC Smith and the obstetrician on call to ABANDON care
of this patient, since she was technically ineligible for care at
LRMC. The ER physicians
disregarded COL Lipsi's order as unsafe, and
referred the patient to Obstetrics which diagnosed and treated the
ectopic pregnancy. LTC Smith further reports receiving an angry,
threatening telephone call from COL Lipsi later that evening
containing the direct order for LTC Smith to turn that patient away if
she should return.
CASE #2: September 1994 - 60 year old female with disorientation,
generalized contusions, suicidal depression, and without anywhere to
go. The LRMC ER reportedly held the patient as too unstable to
discharge; after x-rays ruled out the presence of fractures, The
patient was referred by LTC Smith to the general surgeon on call, and
was seen by Social Work Chief LTC Robichaux and admitted by LRMC
Psychiatrist Dr. Alfano. COL Lipsi and LTC Gillingham reportedly
reprimanded LTC Smith for treating this patient. COL Lipsi is quoted
as telling LTC Smith during the reprimand session that GEN Kiley had
ordered a punitive deduction from LTC Smith's paycheck to pay for the
patient's care.
CASE #3: February 1995 - an elderly female with dehydration,
orthostatic hypotension, loss of consciousness and altered mental
status. LTC Smith reportedly received an angry direct order from COL
Lipsi to discharge this patient, while COL Lipsi remarked, within
hearing of all of LRMC ER nursing staff, especially CAPT Cape, CAPT
Lamer, MAJ Sandstrom, SSG Marmann, SSG Gaines, SSG Barrett, and TSGT
Bulger, that LTC Smith was to pretend that Landstuhl was "a rural
hospital in Kansas," and to put the patient back into her car and
tell
her to go to a German hospital. The report verifies that the ER
personnel did not obey COL Lipsi's order but instead continued IV
fluids and monitoring as well as cervical spine precautions, and
stalled until the Liaison Representative was able to arrange an ALS
ambulance transfer to a local intensive care unit.
CASE #4: June 1995 - MAJ Brian Lein, General Surgeon, is reported by
LRMC ER personnel to have received an unlawful direct order from COL
Lipsi to send home a 15 year old boy with post operative sepsis.
Accusations against col lipsi & ltc gillingham include forcing 2
physicians, well known by the command to be under psychiatric care for
rapidly worsening major depression, to work in the lrmc er, refusing
them leave time & ignoring their official profiles. Further
allegations are that LTC Smith and LRMC ER Nursing Staff were
reprimanded by COL Lipsi at 0900 on Monday 12 June 1994 for the
lifesaving transfer of a neurosurgical patient, who was in extremis
secondary to brain herniation, to a local Neurosurgical Intensive Care
unit. Other reprisals against ER personnel for requesting adequate
resources to maintain a safe standard of emergency care include a
reprimand session against LTC Smith chaired by GEN Kiley and LTC
Gillingham at 1830 hours on Tuesday 20 June 1994 in GEN Kiley's
office. The reprimands to LTC Smith were reportedly delivered in the
wake of the neurosurgical tranfer in order to intimidate him.
Also reported was the reprisal withholding of awards by ltc
gillingham and col lipsi to two air force physicians because they had
written a memo through their air force chain of command, 86th Medical
Group at Ramstein AFB recommending enhancements to lrmc's emergency
medical service as it became the only emergency trauma center of us
military facilities in europe. Also reported was ltc gillingham's
reprisal withholding of an award from an Army physician who had served
in saudi arabia, because the physician elected to work in the lrmc
emergency room instead of family practice which ltc gillingham headed.
The report alleges that LTC Smith reported in writing the alleged
harassment, unlawful orders, and resulting reckless endangerment by
COL Lipsi and LTC Gillingham to GEN Kiley multiple times in 1995. The
report documents multiple conversations reporting the unlawful
behavior between LTC Smith and other ER personnel and COL Bulliner,
Deputy Commander for Nursing, LtCOL Bodin, Chief of Medicine, and COL
Freyfogle, Trauma Chief.
LTC Gillingham reportedly delivered multiple angry orders to LTC
Smith to force a general medical officer to work as an emergency
physician who had been diagnosed with acute major depression and was
medically forbidden to work in the Emergency Room. One of these
episodes occurred in COL Bulliner's outer office within the hearing of
both MAJ Sandstrom and COL Bulliner. COL Jewett, MC, USA, Chief of
Psychiatry was reportedly notified 7 July 1995 by LTC Smith in
presence of Dr. Darby; COL
Jewett said that he would notify the
Commander and recommended that LTC Smith write a risk management
memorandum for record, requesting GEN Kiley's written guidance,
through COL Lipsi to GEN Kiley, summarizing that LTC Gillingham was
ordering the ER to place on the work schedule a seriously depressed
general medical officer whom MAJ Linda Griffith, USAF psychiatrist,
had recommended not to work in emergency medicine, and that the LRMC
ER was critically short of ER physicians. It is alleged that COL
Lipsi then refused to allow the written memorandum to reach GEN Kiley.
It is alleged that even after these official notifications to the
Command of unlawful orders and reckless endangerment by LTC Gillingham
and COL Lipsi, the unlawful behavior continued.
Dozens of instances of clear violations of the Uniform Code of
Military Justice are alleged against COL Lipsi and LTC Gillingham.
Most involve unlawful orders, deliberate understaffing, and
intimidation, and failure to obey regulations. One report accuses LTC
Gillingham of misappropriating LRMC ER patient workload statistics by
transferring these counts to other clinics. The resulting yearly
patient count applied to the ER was reportedly so falsely low as to
ensure a dangerously low number of ER physicians to take care of the
REAL patient load. It is alleged that patient care was adversely
affected by this misappropriation starting in the Summer of 1995.
LTC Smith reports that both COL Lipsi and LTC Gillingham knew
that he LTC Smith was becoming increasingly depressed. Documentation
is available to show that LTC Gillingham had ordered LTC Smith to see
the psychiatrist MAJ Perotta on call on 17 June 1994 for increasing
depressive symptoms. LTC Smith's report quotes COL Lipsi as
threatening him during the 12 June 1995 reprimand in COL Lipsi's
office, with the following words: "No, LTC Smith, I do not think
that
LTC Gillingham and myself are trying to cause you to have a nervous
breakdown. We do not SHOOT Army doctors who are uncooperative;
however, there are OTHER things that we can do. You do not want to end
up like Dr T_____, do you (referring by name to the former OB-GYN
chief who had earlier sustained a major depression under COL Lipsi's
supervision.)
The IG report alleges that LTC Smith was finally given leave time
off starting 6 September 1995 after five months during which COL Lipsi
and LTC Gillingham had allegedly refused him leave. It is reported
that the Nursing Chain of Command had been aware of the high risk of
situational depression among ER nurses and physicians. Starting in
June 1995, it is reported that COL Bulliner ordered MAJ Mike Kusek,
psychiatric RN, to make rounds on the LRMC ER staff twice daily until
September to guard against suicides among ER nurses and physicians.
Allegedly, MAJ Sandstrom, LTC Williamson, and COL Bulliner are
credited with rescuing LTC Smith from increasing depressive symptoms
by notifying COL Ney Gore, cousin of Vice President Gore and new DCCS
(to replace COL Lipsi ) that LTC Smith needed time off for his own
health. COL Gore is credited with partially protecting LTC Smith and
the ER staff from further reprisals by LTC Gillingham, and with
immediately increasing the resources to the ER toward achieving
standard of care. COL Gore is aid to have initiated many much needed
enhancements to the entire Medical Center.
However, LTC Gillingham's intimidation of LTC Smith and other ER
staff allegedly continued. During the last week of January 1996, LTC
Smith reported to COL Bulliner and COL Gore that LTC Gillingham was
trying to force deployment away from LRMC of three ER physicians
simultaneously. This would reduce the number of ER physicians abruptly
by 50%. On 12 February 1996 at 1300 hours by appointment, LTC Smith
presented a formal IG complaint to GEN Kiley alleging harassment,
unlawful orders, and reckless endangerment by LTC Gillingham and COL
Lipsi.
The IG complaint then alleges that GEN Kiley ordered LTC Smith's
DECREDENTIALING that same afternoon, as well as airevacuation of LTC
Smith one way to CONUS on 24 February 1995. LTC Smith's report alleges
that the medivac was a reprisal for having lodged the IG complaint. The
airevacuation orders were reportedly for major depression, but LTC
Smith reported no specific restrictions in his activities during the
Airevac. In fact, the record shows that letters to members of Congress
were generated on the Airevac computer and printer of Andrews AFB
Medical Center, where LTC Smith stayed; in addition, these letters were
reportedly mailed at the post office at Andrews AFB. The report
continues that as soon as LTC Smith arrived at Madigan Army Medical
Center on 27 February 1996, he was admitted to the in-patient
psychiatric unit. It is alleged
that two days later, the in-patient
psychiatrist MAJ McDonald relayed an order from GEN Kiley to LTC Smith
to move his wife and two school age children immediately on a PCS move
from LRMC to Madigan. Reportedly, the intercession of MAJ Perotta and
COL Gore prevented this abrupt move, and the dependents were allowed to
stay at Landstuhl until school was finished in June. Meanwhile, it is
reported that LTC Smith was kept on in-patient status for three weeks,
at the HIGHEST SECURITY LEVEL 1, because of what MAJ McDonald
repeatedly said was "a delay in clarification of orders from
Landstuhl." A review of the hospital record reports no evidence of
acute depression, only mental and physical exhaustion. LTC Smith says
that his treatment by MAMC hospital staff was exemplary and
compassionate. However, he alleges that the three week duration on
in-patient status at the highest security level was due to reprisal by
the Landstuhl Command, since he was still technically assigned to LRMC
during that time.
These & other serious allegations impacting adversely on the
mission of quality healthcare
delivery, were not investigated by the lrmc ig or the lrmc command.
Consequently, since late february 1996 this complaint has been
investigated by california senators feinstein & boxer &
congresswoman
pelosi.
Author:
COL Allen Rhodes at MEDCOM4_FSHTX
Date:
10/3/97 8:37 AM
Priority: Normal
TO: COL Phil Savoie at MEDCOM11_FSHTX
TO: CPT Jeanette Stone at MEDCOM11_FSHTX
TO: LTC Stephen Smith at MEDCEN4-MAMC
TO: stevewsmith@pol.net at Internet-Mail
Subject: Re[2]: OFFICIAL REPORT TO MEDCOM
JAG & TO MEDCOM CID
------------------------------- Message
Contents -------------------------------
Phil-
As I am taking a day or two off, am working
this one from home. I am
disturbed, to say the least, by LTC
Smith's accusation that the
MEDCOM IG office never instigated an
investigation--they guy is
clearly a few bricks short of a load. I will provide him a reply
next week when I am in the office and have
access to my regulations
and policy documents.
His expectations and reality are not
necessarily the same.
Birds were thicker yesterday than I have
ever seen before, anytime,
anywhere.
See you Monday.
allen
_______________________ Reply Separator
_______________________
Subject: Re: OFFICIAL REPORT TO MEDCOM
JAG & TO MEDCOM CID
Author:
COL Phil Savoie at MEDCOM11_FSHTX
Date:
10/1/97 4:47 PM
Dr. Smith
As I am certain CPT Stone advised you, the
MEDCOM Judge Advocate
office stands ready to assist in any investigation that is initiated
regarding your allegations. The
JAG office does not, however, have
independent investigative authority, as does the CID, IG, commanders
IAW AR 15-6 and AR 40-68 (QA focused) and members of congress. The
JAG office simply cannot initiate an investigation.
We do, however, work closely with those investigative activities and
provide legal support and advice when needed. Undoubtedly, if one of
the agencies finds evidence of wrongdoing, they will consult with my
office for advice on how to proceed further. We stand by to assist in
any way possible. You may feel
free to advise anyone who is
investigating this matter that they may consult with this office.
Philip A. Savoie
COL,JA
Staff Judge Advocate
______________________________ Reply
Separator _________________________________
Subject: OFFICIAL REPORT TO MEDCOM
JAG & TO MEDCOM CID
Author:
LTC Stephen Smith at MEDCEN4-MAMC
Date:
10/1/97 08:35
1 October 1997
COL Savoie
CPT Stone
I appreciate your participation in assisting with my report to COL
Atkinson for LTG Blanck about allegations of unlawful command activity
at my previous assignment. Your help is appreciated since, as my
witnesses reported to me on 6 September 1997, the witnesses reported
evidence of falsification of Medical Records in the neuro-surgical
case of 3 June 1995, as well as diversion of ambulance equipment from
patient care, where it was badly needed to maintain standard of care,
to apparent black market activities which CID is already
investigating.
I have reported to my Members of Congress that I requested THREE
investigations at MEDCOM last week: (1) MEDCOM QA, (2) MEDCOM JAG, and
MEDCOM CID (Agent Patrick Tangarine).
Is there a case # or file # to identify the JAG investigation? If so,
please send it to me for my records, in case the Members of Congress
need more specifics.
I have also reported to the Members of Congress that the MEDCOM
Inspector General investigation was NEVER initiated in regard to
interviews of any of the 65 witnesses. In fact, MEDCOM IG NEVER
interviewed me either by telephone or in person. This failure to
investigate extremely serious allegations involving a Medical Corps
LTC and a COL reporting to and following orders of the overall
Commander, a promotable COL, seems to me also a JAG and CID matter.
LRMC JAG CPT Heller also received a request to investigate on 9
February 1995; however, like LRMC IG LTC Stearns, there was a failure
to investigate.
What other information do you require in order to pursue the MEDCOM
JAG investigation of these matters?
Respectfully,
Stephen Whitlock Smith, MD
Fellow, American College of Physicians
Fellow, American College of Emergency Physicians
LTC, MC
LTG George A. Crocker, USA
Commander
I Corps & Fort Lewis
Fort Lewis, WA 98433-9500
Subject: Article 138, UCMJ
Dear General Crocker,
I am an active duty officer in a tenant
unit at Fort Lewis and I have prepared an Article 138 for filing. I request your personal assistance in this
matter, since I view it as extremely time sensitive.
I am a principal witness in two
investigations directed by the Department of the Army Inspector General. Both investigations center on the reckless
endangerment of patients caused by two Army physicians at Landstuhl Army
Regional Medical Center (Germany) between 1993 and 1996. These physicians were following the explicit
orders of then Colonel Kevin Kiley, MC who now serves as a Brigadier General in
the Office of the Surgeon General of the Army.
As a result of the testimony I have given
in these two investigations, I have been compelled by circumstances to report
reprisals taken against me by my commander, BG Mack Hill, and other members of
his command at Madigan Army Medical Center (Military Whistleblower Protection
Act).
I have prepared an Article 138 that I
intend to submit without delay. In his
letter dated 23November 1998 (enc. 1), COL Gerald J. Leeling, DAJA, advised me
to file locally. Following this advice
I visited the installation JAG office on 11 Dec 98, and presented the salient
points of the Article 138 to MAJ Custer, JAGC and CPT Vasquez, JAGC. While attentive, they were clearly
uncomfortable with their own knowledge and somewhat uncertain of how to proceed
with an Article 138.
General Crocker, would you please arrange
an appointment for me with a senior installation JAG officer who has experience
in Article 138 matters? An Article 138
filing is a serious and complicated undertaking which requires a great deal of
legal and administrative experience.
Further, I ask that you guarantee my right
to the lawyer-client confidentiality privilege and take into account my
expectation of and need for continuous access and advice to this senior JAG
officer for the duration of the proceedings that flow from the filing.
During duty hours I can be reached at
968-3866 (DSN 782-3866).
Respectfully,
Stephen Whitlock Smith, MD
LTC, MC
Department of Medicine
MAMC
ENCLOSURE 1 (2 Pages)
NOTHING FOLLOWS
TO PERSONAL ATTENTION OF:
LTG Ron Blanck
Surgeon General of the Army (HQDA
(SGPS-PSQ), Skyline 6, #672,
5109 Leesburg Pike, Falls Church, VA
22041-3258
(703) 681-3000
10 June 1999
LTG Blanck:
I am enclosing a copy of my long pending
Washington State Verification and Evaluation of Privileges which Madigan
Commander BG Mack Hill has still not signed. Without this verification, I am
unable to obtain the Washington State Medical License and seek civilian
employment.
LTG Blanck, I am therefore appealing to
you directly to verify my privileges
and send the signed form directly to WASHINGTON STATE MEDICAL QUALITY ASSURANCE
COMMISSION.
I am also enclosing your copy of my
original FAX request to you for early retirement, so that you will have a
better copy for your records.
Respectfully,
Stephen Whitlock Smith, MD, LTC
Telephone Voicemail (253) 968-3866
E-mail stevewsmith@pol.net
Cc:
Sen. Thurmond, Rep Spence, Rep Stark
Washington State Medical Quality Assurance
Commission
Drs. O'Leary, Buck, Lee; Mr. Gaffney, Mr.
Johnson
25 May, 1999
LTG Ron Blanck:
The Surgeon General of the Army
Commander
MEDCOM
Fort Sam Houston, TX
210-221-7118
1. I
request retirement from active duty effective 30 June 1999, and placement on
the retired list effective 1 July 1999.
I request an early retirement based on my length of service, and
constructive credit based on my quality management reports to higher
authorities in lieu of Command and General Staff studies. I anticipate no medical condition that would
result in other than a routine length of service retirement.
2. I
request that I be placed immediately into an ordinary leave status until the
balance of my account is exhausted and then to continue in an advanced leave
status until my retirement becomes effective.
3. I
request that my local MTF and other credentials files and privileging records
and any reports to licensing authorities reflect an unrestricted unsupervised
Category III in Internal Medicine.
4. I further request that when my local
MTF and other credentials files and privileging records reflect an
unrestricted, unsupervised Category III in Internal Medicine, any and all local
or other administrative processes involving the restoration of my clinical
credentials be terminated.
Stephen Whitlock Smith, MD, LTC
Telephone Voicemail (253) 968-3866
E-mail <stevewsmith@pol.net>
NOTHING FOLLOWS
LTG Blanck:
I am
thankful for your decision of 14 May to accept my credentials appeal, which I
am enclosing. Our past association is two-fold:
* I am the Army-trained doubly-board
certified Army physician who leads your Telemedicine Special Response Team for
Madigan Army Medical Center; and,
* I am the former Emergency Medicine Chief
at Landstuhl Regional Medical Center who as LRMC's Joint Commission (JCAHO)
Liaison for Medical Staff filed a report critical of then COL (P) Kevin Kiley's
Command for alleged reckless endangerment of patients and staff.
Your personal intervention has served well
in the past. Your QM Team recommended an investigation in October 1997.
However, as the European phase of the investigation began in summer of 1998, I
found myself to be targeted with apparent reprisal actions by BG Mack Hill, MAMC's
new Commander.
The reprisals have included BG Mack Hill's
reported confrontation with anger apparently directed at me followed by my
alleged forced detention by a Hospital Security Chief after I spoke briefly with
Dr Sue Bailey, Assistant Secretary of Defense for Health Affairs, in the
receiving line. More recently, BG Hill has summarily suspended my credentials
to practice medicine in a series of credentials actions apparently at variance
with due process protections under JCAHO and Army Regulations.
My credentials were restored on 3 March
1999 by a vote of my fellow physicians on the Credentials Committee, then again
by means of memorandum by then Acting Deputy Commander COL Kelly and by my
physicians However, BG Hill has delegated further action to his JAG attorney,
including the threat of legal action via Army Regulation 15-6, a precursor to
court-martial.
While I have been forced to skirmish over
credentials with BG Hill, the investigation in Germany seems to have faltered.
COL David Lipsi and LTC David Gillingham were named in my allegation that they
ordered my ER staff to abandon care of unstable civilian patients on strict
eligibility criteria and that we suppress adverse QA data (against JCAHO and AR
guidelines). We refused those orders, and reprisal followed. Both officers
alleged that they were following specific direction from then COL (P) Kevin
Kiley. LTG Blanck, would COL Lipsi be retiring under current DOD guidelines if
the investigation were progressing?
I have tried to remain on active duty long
enough to see the investigation through which I help to trigger, along with my
witnesses, because we do not wish to see vulnerable and sick patients
endangered by what we considered to be reckless leadership at LRMC. I find it very difficult to serve
efficiently within your organization until these hazards have been recognized
via formal investigation, and remedied.
When I gratefully accepted the Army's
offer for medical scholarship at George Washington University School of
Medicine in 1977, I considered whether I would ever be subject to unlawful
orders that could endanger patients. After many years as an Army doctor, I
found myself for the first time refusing to carry out orders by COL (P) Kiley's
subordinates that I knew would harm unstable patients under my emergency care.
I then found myself under apparent reprisal credentials actions similar to what
Joint Commissioner examiner Dr Bert Hurowitz had reported previously. COL David
Lipsi allegedly issued reprisal against 3 LRMC physicians who had filed reports
with Dr Hurowitz. Known alleged deficiencies in emergency and other equipment
and procedures were reported to COL (P) Kiley who arrived at LRMC several
months later. Yet, COL Kiley instead chose in my opinion to hide evidence of
JCAHO noncompliance and to issue reprisals against those who recommended
adherence to standard of care.
One of the patients that I reported as
harmed lives within the region represented by Senator Strom Thurmond and by
Representative F Spence. An appeal is made to them to allow investigation of
COL Lipsi before his retirement at Fort Jackson South Carolina, so that BG
Kiley's alleged involvement in the apparent cover-up of case is made clear.
Only your personal intervention, LTG
Blanck, will now resolve this situation. You will also require the assistance
of outside organizations.
I therefore request of you the following
actions in order to prevent harm to more patients, and reprisal against those
who report such harm:
* Exclude BG Kevin Kiley, who now works for you in the Surgeon
General's Office of any influence in over the military and medical careers of
myself and the other witnesses in the multiple Federal investigations stemming
from my original Inspector General Complaint;
* Similarly exclude BG Mack Hill, since he
serves well within the sphere of influence of BG Kevin Kiley, from recent past
association as well as present day-to-day business;
* Afford me due process in completing full
restoration of my medical credentials in conformity with JCAHO and AR
standards.
* Please consider my application for early
retirement, now pending since I became eligible last November.
Thank you for your attention,
Stephen Whitlock Smith, MD
FACEP, FACP
Lieutenant Colonel, US Army Medical Corps
Madigan Army Medical Center, B310-904
MAMC, Pendleton Avenue, Tacoma, WA 98431
(253) 968-3866 stevewsmith@pol.net
Cc:
Members of Congress, including Sen.
Thurmond, Rep Spence, Rep Stark
Mr. Cohen, Mr. Caldera, Dr Bailey
Generals Reimer, Crocker
Drs. O'Leary, Buck, Lee
Mr. Gaffney, Mr. Johnson
Ms Jowers, Mr. Ramsey, Mr. Timms, Mr.
Siceloff, Mr. Parker, other correspondents
Agencies
Stark Analysis Shows Weakness in JCAHO
Audits,
Calls for Overhaul of Hospital Review
Process
"Unsafe conditions and unacceptably
high death rates are too often present in hospitals ranked as excellent by the
Joint Commission for Accreditation of Healthcare Organizations (JCAHO),"
Rep. Stark announced today. California's Health and Welfare Agency shows high
mortality rates among JCAHO-accredited hospitals, and a report just issued by
the New York City Public Advocate documents unsanitary conditions in hospitals
with high scores.
Rep. Stark compared the California public
health agency's list of survey results with JCAHO's list of accredited
hospitals. He found 29 JCAHO-approved hospitals had higher-than-expected death
rates for heart attack patients, some as high as 30-40%. "This means that
patients may have a one in three chance of dying from a heart attack, even
though they make it to the hospital, yet two of these hospitals received
JCAHO's highest rating," Rep. Stark said.
California's report is the third published
since 1993 that compares mortality rates from heart attacks across hospitals
and controls for a variety of factors, including patient age, sex, type of
heart attack, and chronic diseases.
In a separate analysis of New York
hospitals, the non-profit Public Advocate presents strong evidence that
hospitals circumvent JCAHO's annual announced survey visits -- simply by hiring
extra staff to make operations look smoother than they really are.
In too many cases, the report finds that
JCAHO's high test scores mask a darker reality -- that some accredited
hospitals don't meet basic standards of care. For example, 15 accredited
hospitals showed problems ranging from substantial delays in treatment of
emergency room patients to outdated and broken equipment to overcrowded,
understaffed clinics and unsanitary conditions.
"Clearly, when such conditions are
present, JCAHO should respond with sanctions, not high praise," Rep. Stark
said. "Yet only last year, JCAHO flunked fewer than 1% of hospitals. The organization
says that it fails so few because it prefers to work with hospitals to
'correct' any violations that are detected. But if its accreditation standards
are low to begin with, then can consumers and plans really rely on JCAHO
reports?" This is a critical question for Medicare beneficiaries, since
JCAHO-accredited hospitals are "deemed" to have met Medicare's
"Conditions of Participation," a key proxy for quality of care.
The weaknesses of JCAHO's current system
are made plain in the New York report. Simply put, there are no surprise
inspections, and little apparent follow-up of pro-forma walk-throughs.
To make matters worse, under the Joint
Commission's arbitrary scoring system, hospitals with serious quality of care
problems are often given excellent ratings. In effect, JCAHO surveyors are
encouraged to rank hospitals highly on each standard, even if the hospital is
unable to meet that standard! This practice makes a mockery of the review
process.
"I am astounded that of the 18,000
institutions surveyed each year, none are judged to fail outright," Rep.
Stark said. In fact, ALMOST ALL (98 percent) of the institutions surveyed in
the New York City study received scores of 80 or better on a 100 point scale,
and NONE had a score below 70!
"The misguided scoring and lax
oversight documented in the New York and California reports suggests that
another system of oversight is needed. I am cosponsoring two bills that would
overhaul the current voluntary review process," Rep. Stark said. The
Accreditation Accountability Act of 1997 (H.R. 800) would require all
Medicare-accrediting organizations to hold public meetings. One-third of
governing board members would be members of the public.
Second, the Medicare and Medicaid Provider
Review Act of 1997 (H.R. 2543) would levy user fees on hospitals and other
health care providers to underwrite the costs of independent federal compliance
and audits. President Clinton included the heart of this bill in the budget
package he recently sent to Congress.
"For too long," Rep. Stark said,
"we've given JCAHO and the health care industry the benefit of the doubt.
Self-policing simply isn't working. The New York City report is all the
evidence we need to show that patients suffer -- sometimes fatally -- from
substandard care provided by JCAHO-accredited hospitals. Let's put patients'
needs first, back where they belong."
Contact: Anne Montgomery
25 May, 1999
The Surgeon General of the Army
Commander
MEDCOM
Fort Sam Houston, TX
210-221-7118
1. I
request retirement from active duty effective 30 June 1999, and placement on
the retired list effective 1 July 1999.
I request an early retirement based on my length of service, and
constructive credit based on my quality management reports to higher
authorities in lieu of Command and General Staff studies. I anticipate no medical condition that would
result in other than a routine length of service retirement.
2. I
request that I be placed immediately into an ordinary leave status until the
balance of my account is exhausted and then to continue in an advanced leave
status until my retirement becomes effective.
3. I
request that my local MTF and other credentials files and privileging records
and any reports to licensing authorities reflect an unrestricted unsupervised
Category III in Internal Medicine.
5. I further request that when my local
MTF and other credentials files and privileging records reflect an
unrestricted, unsupervised Category III in Internal Medicine, any and all local
or other administrative processes involving the restoration of my clinical
credentials be terminated.
Stephen Whitlock Smith, MD, LTC
Telephone Voicemail (253) 968-3866
E-mail <stevewsmith@pol.net>
NOTHING FOLLOWS
OTHER CASES
INTERNAL MED CHARTS FOR
REVIEW (22 Oct 1998)
From:
Stephen W Smith
<stephen_w.smith@mamc.chcs.amedd.army.mil>
Subject:
INTERNAL MED CHARTS FOR
REVIEW (22 Oct 1998)
MEMORANDUM FOR:
CREDENTIALS AND DEPARTMENT OF MEDICINE
AS REQUESTED FOR REVIEW
COL Les Reed and MAJ Rich
Jordan
FROM: STEPHEN WHITLOCK SMITH, MD
Date: 22 October 1998
As requested, charts are
attached for review, retrieved from computer
records. The others will
follow shortly. (Please see previous memo of 2
October, attached.)
Thank you for streamlining
the Acute Care system. The following improvements
are helping markedly: a)
Allowing us to schedule patients directly with the
primary provider, so that the
acute visit can become more focussed and
shorter, b) allowing
nursing personnel to do a nursing assessment in the
S-O-A-P format, c)
allowing charting time between patients as well as
designating one person to
return charts, bubble sheets, and charts chosen for
audit directly to Dr
Jordan, or Records, or bubble sheet area, whichever is
approriate. All of these
changes seem to cost little in personnel time; these
changes help me personally
to keep up with the work flow, and may be good
innovations to continue
once the 2 Physician Assistants are in place.
The dramatic events
unfolding from the 1 September 1998 visit of Dr Sue
Bailey, Assistant
Secretary of Defense for Health Affairs, which I reported
promptly through official
channels at the time and to Drs Reed, Jordan and
MAJ Rumph as appropriate,
have impacted severely on the time and effort and
effort required to manage
both the important assignment that you have given
me PLUS the required
reporting of harassment clearly intended to silence a
high level complaint. The
details are included in conversations which we have
had recently, as well as
correspondence received in September by Secretaries
Cohen, Bailey and Caldera.
Other government agencies are also investigating,
including a major
investigation just now beginning in the MEDCOM centered on
USAREUR.
I made two requests to
Ernestine Russell for administrative time in early
September in order to keep
up with the increased demands on my time and
energy.
I know that this request
WAS passed on up the chain of command, since it
was mentioned by MAJ Rumph
at the counseling session which took place with
MAJ Jordan. I know now
that the full circumstances underlying my request were
not known to you, since
the Command had not informed you of the 1 September
incident.
I am proud to work for
your Department, and I will try also to be responsible
as well as persistent, in
presenting evidence from my past Command, since
adverse outcomes to
patients did occur there. I reported what I reported in
order that these things
would not occur in other Commands during the drawdown
in resources.
Thank you,
Stephen Whitlock Smith, MD
LTC, MC
MailMan message for
SMITH,STEPHEN W
Printed at
MAMC.CHCS.AMEDD.ARMY.MIL Thu, 22 Oct
1998 07:22:05 (#186)
Subj: INTERNAL MEDICINE
CHARTS: CHCS (02 Oct 1998)
Fri, 02 Oct 1998
16:46:43 229 Lines
From: SMITH,STEPHEN W
(Internal Medicine) in 'DESK' basket.
MEMORANDUM FOR:
CREDENTIALS AND DEPARTMENT OF MEDICINE
AS REQUESTED FOR REVIEW
FROM: STEPHEN WHITLOCK SMITH, MD
------------------------------------------------------------------------------
COMPLETE CLINICAL CHARTS
FOR ALL OF THE PATIENTS SEEN BY ME ARE ACCESSIBLE
UTILIZING THE FOLLOWING
MENUS IN CHCS FOR ALL PATIENTS ON THIS LIST:
1. HEALTH SUMMARY
("MD" TRIPLER SUBMENU
2. PROBLEM LIST (WITH ISD9
CODING)
3. ORDER ENTRY (FOR CLINICAL INTERVENTIONS AS A RESULT OF
THE CLINICAL EXAM)
4. AFTERCARE INSTRUCTIONS
(SPECIFIC FOR DEPARTMENT OF MEDICINE)
5. REFERENCE->PMI (FOR
MEDICATION AFTERCARE INSTRUCTIONS)
PLEASE NOTE:
THIS PROJECT OF ENTERING
ALL CLINICAL ENCOUNTER DATA AT THE TIME OF THE VISIT
IS MORE TIME-CONSUMING
WITH JUST A CHCS VT420 TERMINAL, AS COMPARED WITH A
NETWORKED PC RUNNING
QVT-WINDOWS OR KEA! (THE ALTERNATIVE PROGRAM).
HOWEVER, THIS ORDER-ENTRY
(ESPECIALLY USING THE UPDATED CHCS DESKTOP) CREATES
A PERMANENT RECORD
ACCESSIBLE BY ALL MAMC PHYSICIANS AND PA'S AND NURSE
PRACTITIONERS FROM THE
DESKTOP. THIS PROJECT WAS UNDERTAKEN WITH THE HELP OF
THE NURSING STAFF OF APCC,
AND IS EVOLVING. THE RATIONALE OF ITS USE,
PARTICULARLY FOR THE
ACUTE-CARE PORTION OF THE ADULT PRIMARY CARE CLINIC, IS
THAT IT WILL BE VIRTUALLY
IMPOSSIBLE FOR THE SAME PROVIDER TO SEE ONLY THOSE
PATIENTS ASSIGNED TO HIM OR
HER; AT LEAST WITH A NETWORKED ELECTRONIC RECORD
LIKE THIS ONE, OR LIKE THE
ONE IN PROGRESS BY LT KAITANI AND ALSO BY EPIC
SYSTEMS (WITH OR WITHOUT
VOICE MACRO COMMAND INPUT), ANY APCC PROVIDER COULD
ACCESS ALL CLINICALLY
RELEVANT DATA WITHOUT WAITING FOR THE PAPER RECORD,
EVEN IF IT IS AVAILABLE.
SINCE MY SCHEDULE IS KEPT
FREE FOR ACUTE VISITS AND TELEPHONE CONSULTS, THERE
IS NO TEMPLATE WHICH WOULD
ALLOW REVIEW OF MY RECORDS ARRANGED BY DAY OF
VISIT, CHRONOLOGICALLY.
THIS LACK OF TEMPLATE, A
NECESSARY SITUATION AT PRESENT, HAS MADE IT
DIFFICULT TO ACCESS ALL OF
MY CHARTING FOR ACUTE CARE WITHOUT USING A
SEPARATE LIST OF ALL
PATIENTS WHICH I HAVE SEEN DURING ANY FIXED TIME PERIOD.
IF MY CHARTS ARE REQUIRED FOR
REVIEW AT ANY TIME, PLEASE ASK ME OR THE ACUTE
CARE TEAM FOR A COMPLETE
LIST OF MY PATIENTS.
STEPHEN WHITLOCK SMITH, MD
LTC, MC 024-38-5114
Followup Scheduling:
(253)968-2410/2415
Questions: (253)968-3866
Beeper; # PENDING
E-Mail: <stevewsmith@pol.net>
Mailing address: Adult Primary Care Clinic
MAMC, PENDLETON AVENUE,
TACOMA, WA 98431
[PAGE]
Subj: INTERNAL MEDICINE CHARTS:
CHCS (02 Oct 1998)
Patient names are edited
out
Local Message ID:
5281549@MAMC.CHCS.AMEDD.ARMY.MIL
MITH,STEPHEN W (Internal
Medicine) Last read: Thu, 22 Oct 1998 07:21:50
STEVEWSMITH@POL.NET Sent: Fri, 02 Oct 1998 16:50:41 Time: 6
seconds.
Forwarded by:
SMITH,STEPHEN W Fri, 02 Oct 1998 16:48:36 through
response
0.
REED,HARRELL L (Chief, Department
of Medicine) Last read: Fri, 09 Oct 1998
15:48:55 Forwarded by:
SMITH,STEPHEN W Fri, 02 Oct 1998 16:51:03
JONES,D E CASEY Not read. Forwarded by: SMITH,STEPHEN W
Fri, 02 Oct 1998
16:51:03
JORDAN,RICHARD A (Chief,
Internal Medicine Services.) Last read: Mon, 05 Oct
1998 16:26:01 Forwarded
by: SMITH,STEPHEN W Fri, 02 Oct 1998 16:51:03
[PAGE]
18 Mar 99
Memorandum for Credentials Committee
Subject: Proctor and Supervision Program for LTC
Stephen Smith (024-38-5114) (Original memo submitted 15 Mar 99 and revised 17
Mar 99 per Committee)
(Revised 25 March per Chair Committee)
1. As a result of the recent credentials hearing
held on 3 March 1999, this memorandum and the associated proctorship and
Supervision Program is being submitted to the Credentials Committee. The
proctorship and Supervision Program contains the following areas which will be
outline in the memorandum below. Part I: Supervision of LTC Smith, Part II:
Daily chart review of medical records by LTC Smith, part III: Daily feedback to
LTC Smith regarding both direct observation and chart review, Part IV:
Progression to relief of supervision status based upon a specific, successful
display of documentation, Part V: Standardized chart entry using a handwritten
format and a DA 600 overprint, Part VI: Supervisory chain of authority for a)
administrative supervisor, b) clinical review supervisor and c) functioning
clinical supervisor.
a. Part I. Direct supervision of LTC Smith: For the
first five days of the initiation of this Proctorship and Supervision program,
LTC Smith will be directly observed with every patient interaction that he has.
Direct supervision will be carried out by the Chief, Department of Medicine or
his designee to include a senior internist at the rank no less than LTC. The
evaluation and feedback of these direct supervision periods will be carried out
in the same way that the daily chart reviews will be carried out and listed in
the paragraph below.
b. Part II. 100% Chart Review: During the entire
time of the Proctorship and Supervision Program, 100% of LTC Smith's medical
records documenting the interaction with patients will be reviewed until a
sequential reduction in the % reviewed may occur as in paragraph 1d. These
reviews will not include telephone consults or consultation to subspecialty
services unless the daily chart evaluations suggest that important patient
management information is contained in consults or telephone records. This
chart review will be carried out using a standardized format, using the
template which had previously been used to review LTC smith's charts and the
control group in the fall of 1998. The person designated to review these charts
will be LTC Curtis Hobbs, Department of Medicine Quality Assurance Coordinator.
If LTC Hobbs is not available, LTC Spencer Root, Department of Medicine risk
Management Representative, will carry out these reviews. if neither of these
two individuals is present and available, then the Chief, Department of
Medicine, COL H. Lester Reed, will carry out the daily chart reviews. the
outpatient medical record and research files for review must be placed in the
designated area by 1900 hours on the day of the afternoon clinic visit and if
only morning clinics are scheduled, then by 1500 hours in the same site. A specific designated area which will be
accessible to the three individuals mentioned in this paragraph will be
determined, and this site clearly identified to LTC Smith in a written memorandum
describing the proctorship and supervisory program. Provider evaluation
feedback will be delivered daily on aspects of care beyond chart documentation
as identified in Para 1c. If these evaluation forms suggest areas of
improvement such as with consults or telephone communication then these
documents will be reviewed regularly until they meet compliance limits as
outlined in Para 1d.
C. Part III. Daily feedback to LTC Smith. By the
close of business (1730hrs) on the day following the patient encounter, a
standardized feedback sheet will be provided for LTC Smith which will review
the deficits and correct entries for the summary of the previous day's medical
records. The Medical Feedback Sheet will also include several other items in
addition to documentation, such as a treatment plan evaluation, apparent depth
of medical knowledge and patient interaction sections. The medical records will
also b given a screen for appropriateness of medical care and this feedback
will be entered on the daily sheet-These feedback sheets will be electronically
produced by the reviewers and will be of a standardized template form currently
modified from residency training forms. A specific area for documenting areas
to be improved will be present and if no suggestions appear in this box, it can
be assumed that the medical records meet/are within variation for a peer group
mean. This evaluation holds LTC Smith to an acceptable medical record review
for there to be no comment entered.
D. Part IV. Progression to Relief of Supervised
Status. Based upon the successful display of documentation for all elements
originally reviewed in the records, the chart review frequency will be modified
in a sequential manner. The elements of the standard documentation review form
used by LTC Hobbs and LTC Root in 1998 will be tabulated as 'met' or 'not met.'
A mean score will be generated from these sheets for the aggregate of all
charts for that day. This mean must be within two standard errors of the mean
(SEM) for the peer reference group in order to not be called different. Failure to be similar to a control peer
group will delay the reduction in chart review frequency which is described
under the guidelines of this Proctorship and Supervision Program. Repeated
failure to meet the documentation standards as outlined in this Proctorship and
Supervisory Program and recommendations to the Credentials Committee with
regard to privileging. A comparison to a concurrent peer group will be made
using the same standardized review sheet and a two SEM difference between these
two groups will be determined as a maximum allowable documentation variation.
This SEM will be calculated based upon the specific elements of the
documentation review sheet. Under this program, a sequential reduction in
charts being reviewed will proceed if successful completion of the
documentation elements has been met and records are within 2 SEM's of the peer
group on other measures as noted above. After 30 days of supervision and
successful completion of the Proctor and Supervision Program, a reduction to
50% of charts being reviewed will be recommended without supervision. After 60
days of successful proctorship with the Proctorship and Supervision Program, a
reduction to 25% of charts being reviewed will be recommended without
supervision and after 90 days of successful Proctorship and Supervision
Program, privileges for Internal Medicine will be recommended without
supervision. The failure at any time to consistently meet the documentation
standards over a five-day workweek will revert this Proctorship and Supervision
Program to the beginning of the supervision period, and will generate a report
to the Credentials Committee. It should also be noted that the clinical
management of these cases will be reviewed along with the documentation. The
clinical management will be reviewed in a way consistent with the quality
assessment management currently carried out for similar patients, and a
repeated 'Fail' on this form over a five day workweek will also generate a
report to the Credentials Committee.
E. Part V. Standard Chart Forms. The standardized
chart forms for the use in the acute care setting will be used by LTC Smith for
every patient encounter. These standardized forms will have identified areas
for completion and they will be handwritten. No use of electronic equipment
will be authorized for the completion of these standardized forms. This
requirement is necessary because of the need to have accurate paper
documentation for entry into the medical record and a timely review by the
individual staff members.
F. Part VI. Supervision of Specific Sub Area
Delineation. LTC Smith direct supervisor for administrative actions will be COL
Mark Crowe who is his current rater and, an alternate direct supervisor will be
his senior rate COL H. Lester Reed, Chief, Department of Medicine; his
supervisor for the clinical review of the records will be LTC Curtis Hobbs as a
primary supervisor, LTC Spencer Root as an alternative supervisor, and COL H.
Lester Reed as the reviewer and supervisor if these two are not available. The
clinical function supervisor involved with direct patient assignment will be
COL Howard Cushner and if he is not available, COL H. Lester Reed, Chief,
Department of Medicine will serve in this capacity. The specific supervisory
delineation roles will be outlined to each of the individuals prior to the
initiation of this Proctorship and Supervision Program.
2. The specific area for this proctorship and
supervision program will be delineated in the Adult Primary Care area and will
involve the acute management of the patients seen in that area. Additional
duties for LTC Smith which are not involved with patient care will include
Administrative items not pertinent to this review.
3. An update
on this Proctorship and Supervision Program will be submitted to the Credentials
Committee on a monthly basis and it will include no less than the documentation
reviews, feedback analyses and finally, a recommendation to advance to the next
level of relief of supervision.
4. The final revisions are underway for the 1)
Standard Encounter Form, 2) Daily Evaluation Feedback Form and 3) written
instructions to LTC Smith outlining the program. When these are complete, they
will be submitted to the committee for review, if desired.
Dr. Hickey's letter
October 13 1999
Dennis O'Leary, MD
President, Joint Commission on Accreditation of
Healthcare Organizations
One Renaissance
Oakbrook Terrace, IL 60181
Dear Dr. O'Leary:
This letter is written at the request of Stephen
Whitlock Smith, MD who is currently assigned to Madigan Army Medical Center in
Tacoma, WA. Dr. Smith appears to have a legitimate complaint regarding
Madigan's (MAMC) handling of his credentials which has potentially devastating
effect on his ability to maintain his licenses and earn a living. LTC Smith was
transferred to MAMC from Germany where he had lodged formal complaints against
his command structure. LTC Smith was treated by MAMC for depression. As part of
the treatment of his depression, formal psychometric testing was performed in
March of 1997. The test results which were formally reported to the impaired
provider committee and credentials committee appeared to have been manipulated
to represent LTC Smith as being severely impaired, but which in review years
later were read to be "normal."
These records and reports since that time have
"disappeared." LTC Smith, furthermore, was formally charged/diagnosed
as being "psychotic" by LTC Fred Johnstone, an orthopedist and
chairman of the Madigan Healthcare Provider program which was further used to
restrict/limit LTC Smith's credentials without the benefit of any psychiatric
evaluation or opinion. LTC Smith was being seen at that time in therapy without
ever having displayed any traits which could be construed as being psychotic.
LTC Smith has had various observations, accusations attached or included in his
formal credentials file which are totally inappropriate and slanderous in
nature.
I do feel that in many regards, LTC Smith's rights
have been sorely abused under the JCAHO standards for due process concerning these
matters, the Army Regulations 40-68 Medical Quality Assurance, Army Regulation
15-6 hearings and Committees, and the DOD directives concerning whistle
blowing. I do feel that JCAHO should investigate these occurrences as it seems
to represent an extremely authoritative bureaucracy which was abusive and
destructive in its powers.
If I can be of any further assistance, please feel
free to contact me at the above address or phone number.
Sincerely,
Deborah Hickey, D.O.
Colonel, Medical Corps (RET), US Army
END OF DRAFT VERSION OF JCAHO19991116
Dr. Denise Kirkland
AFFIDAVIT
Little Rock AFB, AR. USAF
Hospital. Dr.
Denise Kirkland.
Internal medicine physician who entered the Air Force out of
private practice. Alleges
unwarranted letters of reprimand,
letters of counseling, unfavorable information file, referral
of officer performance reports, loss of physician bonus, loss of
a retroactive promotion to major, and commander directed
psychiatric evaluation for identifying substandard care at
the USAF Hospital, Little Rock.
She filed suit in Federal
Court for a Writ of Habeas Corpus relating to her contract.
Judge dismissed the case because she did not appeal to the AFBCMR
even though the law did not require it.
She appealed to the AFBCMR to resign her contract and was denied. An appeal was filed in Federal Court and was
also denied. She was recently accused
of refusing to treat or care for a
critically ill patient while her, Dr. Kirkland's, dominant
hand was in a cast. Her
privileges were suspended without a
hearing and she was given an Article 15. She refused the Article 15 and demanded a trial by
court-martial. The trial is set for
September 9, 1991 at Little Rock AFB, AR.
Her husband, David, has made contact with ABC News Prime Time, Newsweek,
Time, U.S. News, New Physician, U.S. Medicine,
American Medical News, New York Times, and The Washington
Post. David spoke with Mr. Upschulte
from Senator John Glenn"s office and Upschulte told him that his wife
could file a Federal Tort Claim for slander and libel. Upschulte also said that any military member
can have court-martial charges brought against another member, regardless of
rank or position, if they go through their major command and can prove the
allegations.
"A Current Affair" showed Representative Barbara Boxer
discussing this case. Dr. Kirkland won
her case against her Air Force accuser.
She has left the Air Force.
Morgan Welsh, LL.B. attorney for Dr. Denise Kirkland, 501- 376-9900. 620 West 3rd street, suite 100, 3685 Little Rock, Arkansas 72203. Fax:
501-376-3724.
Dr. Voge's SWORN STATEMENT: Eugene Fidell,
LL.B. is Dr. Voge's attorney:
202-466-8960.
I was a "rising star" in the Navy's flight surgeon
program until I was assigned as the only medical officer at the Navy's Safety
Center in 1978. The mission of my
particular office was to analyze aircraft mishaps to determine
medical/physiological/psychological causes and contributing causes. At that
time, alcohol, drugs, fatigue, circadian rhythm problems and the like, although
very prevalent causes and contributing causes of aircraft mishaps, were not
officially accepted. The line admiral
for whom I worked at the Safety Center was very safety conscious. He endorsed our findings of alcohol, drug,
fatigue, circadian rhythm and other medical problems as causes/contributing
causes of aircraft mishaps. Our
findings were widely published. The Navy hierarchy, both medical and line,
became very upset. My admiral was forced
to retire (fired) and I was sent to Guam for"final disposition". Soon
after arriving on Guam, I was found to have serious paranoid personality
problems (the examining psychiatrist later told me he was ordered by the
hospital commanding officer to make that diagnosis, and the Commanding Officer
was ordered to do so by the Bureau of Medicine and Surgery. The hospital commanding officer apparently
was promised he'd be made admiral if he were to cooperate). Since the examining psychiatrist had
a"twinge" of conscious/medical ethics, he referred me to Balboa Naval
Hospital Psychiatry Department for final diagnosis and disposition. The then Commanding Officer of Balboa
Hospital was very much involved in the character assassinations from the Bureau
of Medicine and Surgery I endured at the Safety Center and assured all he would
"take care of" me. After 24
days on a "locked" psychiatric ward, with no facilities for either
females or officers, I was declared not to have a psychiatric diagnosis. (Before leaving Guam for incarceration at
Balboa Hospital, I had secured a promise from a line admiral on Guam, who was
unaware of what was going on in Washington, that, if I were not happy with
Naval Hospital Balboa's psychiatric evaluation, he would ensure I would be re-evaluated
by an Army or Air Force hospital. I repeatedly reminded my Balboa Hospital
captors of this promise.) I then returned to Guam. My Guam hospital commanding officer was extremely upset with the
Balboa Hospital psychiatric results and said he'd "look into"
it. He apparently communicated with
Washington and, within one week of my returning to Guam, I was
decredentialed. The procedures to do so
were not legal and did not follow Navy written policy. I was to be sent to Naval Hospital, Balboa,
for "retraining." I was told
I would not "survive" the training program. (If one who has been decredentialed is not "trainable",
the physician is separated from the Navy.)
I was openly informed my "career (was being) ruined" since I
was not a "team player". I
was encouraged to "save everyone the trouble" and resign my
commission. Being basically very naive
and believing in the "American Way", I chose to fight back. I filed Article 138 of the UCMJ complaints
against my Commanding Officer (my only method of redress in the Navy). I also had the presence of mind to call a
Congressman who arranged for me to be evaluated by the Air Force, at Wilford
Hall Medical Center and the U.S. Air Force School of Aviation Medicine. The Navy was livid. The Air Force found no problems with my
clinical capabilities and found no problem with the treatment I gave my
patients on Guam (the treatment which was supposedly so bad I was
decredentialed.) I have not heard
another word from the Navy about my clinical competence since that time. My legal counsel has maintained I will never
have my record cleared by Navy officials, in spite of the fact the voluminous
documentation we obtained through the Freedom of Information Act clearly
demonstrates the Navy purposely dirtied my records and lied about my clinical
competence and psychiatric fitness. I
was advised I would probably win if I were to go to Federal Court, but that the
Navy would "make (my) life miserable" and try to force me out in the
interim. I first had to go through all the
legal"hoops" in the Navy for redress before I could go to Federal
Court. The process has thus far gone on since mid-1982, and has cost me close
to $100,000.00 of my personal funds. My
case is still pending in Federal Court.
The Navy is attempting to prolong the situation as long as possible,
apparently hoping I will either run out of funds or desire, and give up the
fight. Every commanding officer of each
subsequent duty station I have been assigned to since Guam has assured me he
had "heard all about" me.
Each Commander has been more revengeful and vicious than the last. I have been asked on several occasions why l
don't just "save the Navy the trouble and leave". I have had to endure two more
psychiatric"evaluations". The
Navy cannot understand why I choose to fight back, as no one else does so. I have only survived this long through
Congressional intervention. I will not
leave the Navy voluntarily until my fraudulent record is cleansed. As it is now, every state medical license I
apply for, every hospital to which I apply for staff privileges, and every time
I apply formal practice insurance, I must say I have been decredentialed and
have been an inpatient in a psychiatric hospital. I refuse to leave the Navy with such a fraudulent record.
V.M. Voge, CDR, MC, USN
Rt. 3, Box 73
Gonzales, Texas 78629
21 October 1991
Reprisal: Reporting Pay Fraud Earns 21 Days On Psych Ward Michael Tufariello
Chief Petty Officer
Michael Tufariello (972-492-0464) reports that 600 Reservists were paid even
though they never reported for weekend duty, Dallas Naval Air Station. He eventually received a letter of thanks
and of apology, but not before he was imprisoned in reprisal for 21 days on a
psychiatry ward at Shepard Air Force Base.
Does this inter-service cooperation mean there is a military American
Gulag? He knows of 700 cases of abuse
of military psychiatry, and states that because protective laws are little
known, they are rarely enforced. She
testified before Congress on 19 November 1987 and on 24 March 1988. He has appeared on television ("A
Current Affair" and "Nightline") and been interviewed by Steven
McGonigle, Dallas Morning News (800-431-0010).
His case is known to Senator Barbara Boxer, who champions correction of
such human rights violations. She described
his treatment at the hands of his government as "un-American," and
sponsored corrective legislation which he states was revised in 1993. He testified before Congressional committees
twice: 19 November 1987 and 24 March 1988.
The Senator's aide, Mr. Sean Moore, 202-224-3353, is well-versed in
these issues.
Where were the
doctors' ethics when Chief Tufariello was recommended by his commander for
psychiatric hospitalization? Why didn't
the military doctor simply refuse to hospitalize him after finding him healthy? Would the doctor have been similarly treated
had he refused to imprison Chief Tufariello?
Who was the doctor? Has he read
The Nazi Doctors, by Dr. Robert Jay Lifton?
What means (e.g. ON CALL) of immediate medical-legal assistance, could
be made available for doctors caught in such a moral dilemma?
Times staff writer
WASHINGTON--Military supervisors who use mental evaluations and
psychiatric hospitalization as punishments against service members would face
court-martial and fines of as much as $25,000, under a bill passed by the House
of Representatives.
By a 334-83 vote,
lawmakers moved Sept. 18 to create the safeguards against psychiatric
abuse. The amendment to the 1991
National Defense Authorization Act also directed Defense Department officials
to have an advisory panel of military and nonmilitary experts write procedures
to guide mental evaluations of service members and involuntary psychiatric
commitments to hospitals.
Final approval
will depend on the results of a House- Senate conference on the authorization
act. No equivalent Senate bill
exists. The penalty provisions of the
House bill are opposed by the Defense Department.
Rep. Jim
McDermott, D-Wash., cosponsored the amendment with Rep. Barbara Boxer,
D-Calif., after their offices received several complaints from service members
who said they were being harassed for exposing waste, fraud or abuse within the
military.
"Too often,
whistle blowers have been put through psychological tests, psychiatric interviews,
and even involuntary commitment to institutions, not because they were sick,
but because they tried to tell he truth," said McDermott, who is a
psychiatrist.
In voting to
approve the amendment, House members scrapped a milder recommendation from the
House Armed Services investigations subcommittee that contained no penalties
for psychiatric abuse. The subcommittee
recommendation would have left the issue of regulations for
specific penalties to the advisory committee.
The
Boxer-McDermott amendment would add mental health evaluations and involuntary
psychiatric hospitalizations to the list of personnel actions that may not be
taken without reasonable cause against service members who communicate with a
member of congress, a government inspector general, or any authority in the
member's chain of command.
Under current
law, military whistle blowers are protected against "unfavorable personnel
actions" and against threats to withhold favorable personnel actions. Lawmakers say such language would protect a
member's promotion or assignment, but it might not offer protection against
psychiatric abuse because evaluations and commitments are typically considered
to be medical actions.
Any service
member who "knowingly, willfully and without reasonable cause" forces
another member to undergo mental evaluation or psychiatric hospitalization
would be subject to a maximum $25,000 fine and court-martial, under the House
bill.
To illustrate how
common and severe the military's harassment of whistle blowers can be, Boxer
cited these recent cases:
Robert Finley, a
former Army special forces sergeant who told his superiors that U.S. military
personnel were selling weapons and ammunition on the black market in Thailand.
"What
happened to this gentleman, this hero who came forward? They put him in for psychiatric evaluation
to stop him in his tracks," said Boxer.
"And do you know what the psychiatrist said in this particular
case? 'This is baloney. This man is
perfectly fine. He is telling the
truth. This is being used as a
harassment technique.'"
The former
sergeant has been found fit for duty, and his allegations are now under
investigation by the Defense Department inspector general.
Michael
Tufariello, a former Naval Reserve chief petty officer, who was committed to
the psychiatric ward of a military hospital after he protested payments to more
than 600 Navy reservists who did not show up for training at Dallas Naval Air
Station, Texas.
Tufariello, who
was forced out of the reserves, told his story at a 1987 House hearing. A Navy Inspector General's report concluded
Tufariello suffered "injustices" and cited his superiors for
insensitivity to his rights. The report
also confirmed that reservists received improper payments, but Navy officials
determined it would be impractical to trace the money and get all of it back.
John Reiman,
former chief of anesthesiology at an Air Force hospital in England, was forced
to undergo a mental evaluation after he reported three cases of what he
believed was negligent medical care at the hospital.
The Air Force
inspector general investigated the charges and found problems at the
hospital. Military doctors found Reiman
to be "of sound mind," but he left the Air Force in late 1989 and is
now in private practice in California.
Boxer's amendment to the House bill also tells the
Pentagon to give service members ways to challenge mental evaluations or
psychiatric commitments, and to seek redress when the actions are illegal.
A Pentagon advisory
committee would recommend a set of uniform procedures and protections governing
the evaluations and hospitalizations.
The committee would include military and civilian psychiatrists and
psychologists, military judge advocates and a civilian lawyer, according to the
bill.
In a 15-month
process, the secretary of defense would name the advisory committee members
within 60 days after Congress passes the defense authorization act. The committee then would have six months to
issue recommendations. After taking 30
days to study the recommendations, the Pentagon would send a report to
Congress. Any new regulations to govern
the psychiatric procedure would take effect 180 days after that.
The House
proposal has the support of the
American Psychiatric Association and the American
Psychological Association, the nation's two leading groups
representing mental health professionals.
Defense
Department officials who testified at a March hearing on the whistle blower
protections said the military opposes putting specific language in federal law
that defines mental evaluations or psychiatric commitments as negative
personnel practices. However, the
officials said the services could benefit from clearer regulations governing
involuntary commitments to hospitals.
Rep. Nicholas
Mavaroules, D-Mass., the investigations subcommittee chairman, also opposed the
call for penalties against psychiatric actions because he said they go too far,
too fast.
The
Boxer-McDermott amendment, he said, "would classify all involuntary
hospitalizations as unfavorable personnel actions regardless of whether the
individual needs help.. The amendment would provide criminal penalties...for
seeking the involuntary commitment of a military member. Tut the amendment does not define what is
improper."
In addition,
Mavroules said the amendment overlooks situations where service members commit
themselves
voluntarily. And the
criminal penalties in the amendment, he said, negate the work of the advisory
committee by telling it in advance what conclusions to reach.
But Mavroules
said he agrees that service members need protection against mental harassment,
and that this type of persecution of
military whistle blowers is a real problem.
By Pete Yost
The Associated Press
WASHINGTON--The Army tries to fire a civilian scientist after he
criticizes the Pentagon's "Star Wars" program.
Mental wards used, paper says
DALLAS (AP) -- Some military whistle-blowers have been forced to
undergo psychiatric evaluations and been sent to mental wards as intimidation
or reprisal, a newspaper said Sunday, quoting current and former service
members. The Pentagon denied the
allegations. The Dallas Morning News
investigated 27 psychiatric cases involving the military and found most of the
service members involved had spotless records until they challenged the
system. It didn't say how the cases
were chosen.
The newspaper examined
nine cases in detail in its three-month project.
In one, Capt. Denise
Kirkland, an Air Force surgeon who complained about shoddy practices at the
Little Rock AFB hospital, was told by her supervisor that she had suicidal
tendencies and was ordered to have a psychiatric evaluation in San Antonio.
Another involved Army Staff
Sgt. William T. Murphy, who complained in 1988 about how a friend had been
treated by a superior at the Aberdeen Proving Ground, Md.
A series or reprimands
followed, along with a 30-minute psychiatric examination that reached a
"diagnostic impression" Murphy had passive-aggressive traits. He asked for his record to be cleared.
The newspaper
interviewed Kirkland and Murphy, and examined court documents in Murphy"s
case.
The House Armed
Services Committee has held hearings on psychiatric abuses since 1987 and
continues to prod the Pentagon for reforms.
"It is
intolerable that military whistle-blowers should be intimidated by such an
insidious tactic and that those responsible should go unpunished," said
Rep. Barbara Boxer, D-Calif.
Chester Paul Beach Jr., the Defense Department's acting general
counsel, said the Pentagon is strengthening its policies at Congress"
urging to ensure that psychiatric evaluations are not used against the whistle-blowers."
(via Whistleblower Protection including the
Boxer-McDermott Amendment and through the following Members of Congress:
Senators Thurmond, Boxer, Feinstein, and Representatives Dicks, McDermott,
Pelosi, Spence, and Hyde)